

Background: The concept of clavicle reduction osteotomies for shoulder narrowing is straightforward and fairly linear. A segment of the clavicle bone is removed, the two ends are put together and are held in place by plates and screws so they can heal. But there are numerous details of the procedure which if not precisely done may adversely affect bone healing and could result in a non-union.
One of the technical details is the angle of two bone cuts at the two areas along the length of the clavicle. In theory they should be perfectly perpendicular to the length of the bone. (90 degrees) But the clavicle is not a completely straight bone. It has two curved ends with a straight portion only in the middle. The bone is also angled as it connects the shoulder to the sternum, coming forward and down in so doing. Thus with perfectly perpendicular cuts when the two ends come together they may not fit in a completely contacted fashion throughout the diameter of the bone. A small gap may exist particularly on the posterior surface with the application of the plate and screws.
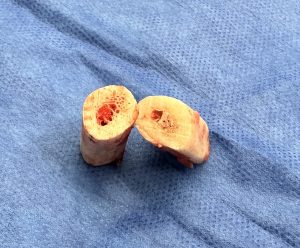
 While angling the bone cuts a bit may ensure complete contact of both bone ends, if a gap develops on either anterior or posterior surface a bine graft should be wedged into it. The removed bone segments provide a ready graft source to do so.
While angling the bone cuts a bit may ensure complete contact of both bone ends, if a gap develops on either anterior or posterior surface a bine graft should be wedged into it. The removed bone segments provide a ready graft source to do so.
Case Study: This young patient desired shoulder narrowing. At 5’ 11” with a bideltoid distance of 52.5cms the goal was a more narrow less square shoulder shape.

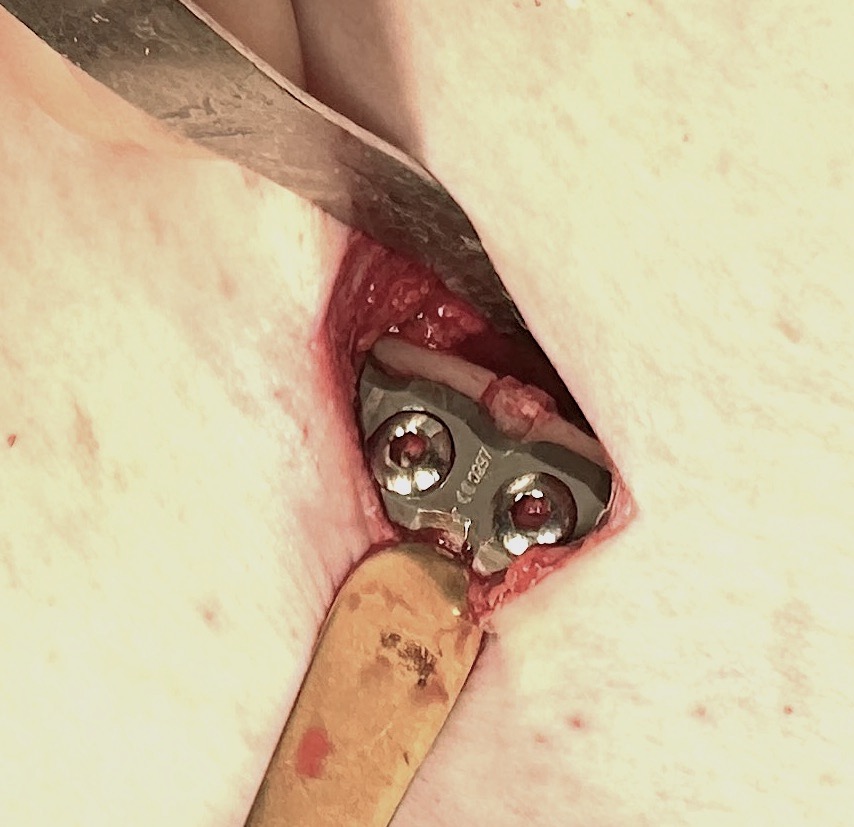
 Under general anesthesia and through 3.5cms incisions in the supraclavicular fossa 2.5cm bone segments were removed with slightly angled bone cuts. In putting together the right side a 2 -3mm gap appeared on its posterior surface after application of the two plates and screws. No such good existed on its anterior surface after application of the anterior plate. A wedge graft was taken from one of the removed bone segments and polled tightly into the posterior gap.
Under general anesthesia and through 3.5cms incisions in the supraclavicular fossa 2.5cm bone segments were removed with slightly angled bone cuts. In putting together the right side a 2 -3mm gap appeared on its posterior surface after application of the two plates and screws. No such good existed on its anterior surface after application of the anterior plate. A wedge graft was taken from one of the removed bone segments and polled tightly into the posterior gap.

 His intraoperative frontal appearance showed the immediate shoulder width change.
His intraoperative frontal appearance showed the immediate shoulder width change.



 Similarly his shoulder appearance seen upright the following day showed similar reductive change in the front and back views.
Similarly his shoulder appearance seen upright the following day showed similar reductive change in the front and back views.
 The postoperative x-ray showed good alignment of the segments on both sides but the wedge bone graft could not be seen.
The postoperative x-ray showed good alignment of the segments on both sides but the wedge bone graft could not be seen.
 It may seem contrarian to be placing a bone graft into a reduction osteotomy site but it does not add back any length. Ensuring optimal bone contacts between the two bone ends is the most assured method to optimize bone healing and prevent a non-union. The convenience of obtaining a graft from the removed bone segments makes this an obvious choice to do.
It may seem contrarian to be placing a bone graft into a reduction osteotomy site but it does not add back any length. Ensuring optimal bone contacts between the two bone ends is the most assured method to optimize bone healing and prevent a non-union. The convenience of obtaining a graft from the removed bone segments makes this an obvious choice to do.
Key Points:
1) In clavicle reduction osteotomies the reapproximation of the two cut ends may not always create a complete circumferential end to end union due too slight differences in the angle of the bone cuts.
2) If there is any gap between the two ends on the posterior side of the bone a wedge bone graft can be placed which is tapped into position.
3) The absolute necessity for a wedge graft in an open clavicle osteotomy side is unknown but a bone graft already exists to use.
Dr. Barry Eppley
World-Renowned Plastic Surgeon