

Background: One of the main aesthetic proportions involved in facial beauty is that of the facial thirds. This is based on the concept that the face is divided into horizontal thirds. The upper third is from the hairline to the glabellar region between the eyebrows, the middle third is from the glabella to the base of the nose (subnasale) and the lower third is from the subnasale to the bottom of the chin. (Menton) While ideally the vertical length between these facial thirds should be exactly equal it rarely is. But as a general concept it helps aesthetically beneficial if they are relatively close in vertical lengths.
There are some gender differences in the facial third concept in that for men, due to the larger size of the lower jaw (lower facial third) which is often considered a sign of increased masculinity, a larger lower third of the face is acceptable. This is why when in the male the lower third of the face is vertically deficient it is aesthetically very noticeable….something just looks off. While it may be recognized there is a jaw deficiency, the vertical jaw deficiency whether not is the chin or the entire jawline is often under diagnosed.
The reason the short lower third ion the face or the vertical jaw deficiency is under diagnosed is that there are seemingly so few options to treat it. Lack of knowledge of how to treat it makes its recognition unlikely. Isolated vertical lengthening of the chin can be done by an opening wedge bony genioplasty or a vertical lengthening chin implant. But lengthening of the entire jawline is not as well known.
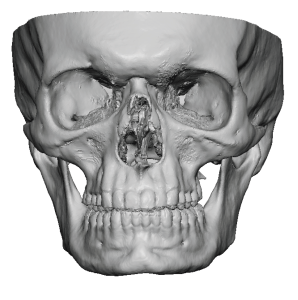
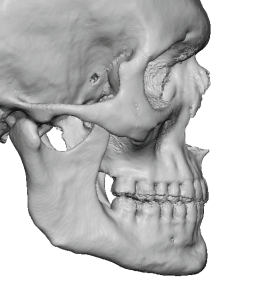 Case Study: This male presented with a desire for a stronger jawline. On examination he had a short lower facial third with a flat mandibular plane angle. While he would benefit by some horizontal chin projection and increased jaw angle widths, what he was more deficient in was int vertical jawline length. His 3D CT scan demonstrated the vertical shortness of the lower jaw.
Case Study: This male presented with a desire for a stronger jawline. On examination he had a short lower facial third with a flat mandibular plane angle. While he would benefit by some horizontal chin projection and increased jaw angle widths, what he was more deficient in was int vertical jawline length. His 3D CT scan demonstrated the vertical shortness of the lower jaw.
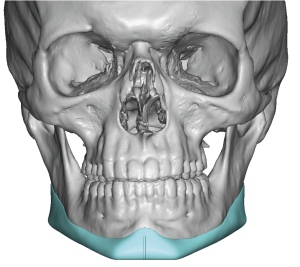
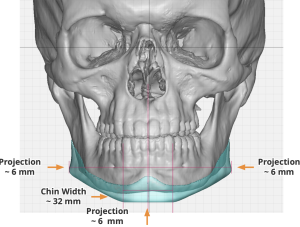
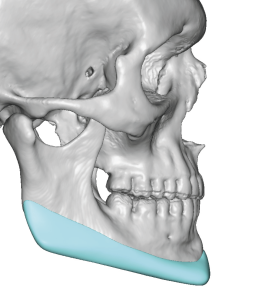
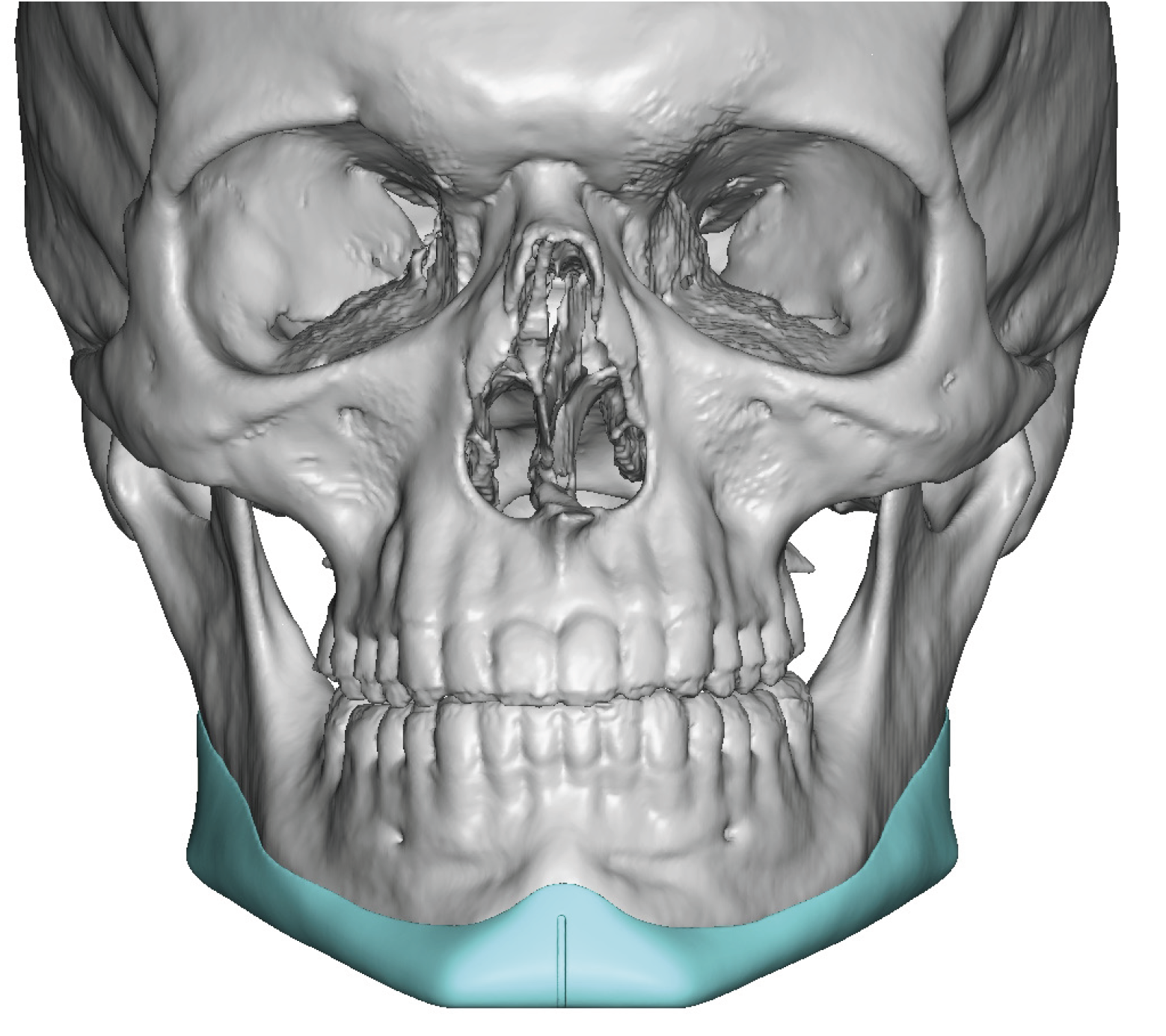
 Using the 3D CT scan a custom jawline implant was designed that added some modest horizontal chin projection and jaw angle widths. But the greater augmentation effect by surface areas was along the entire jawline dropping down its inferior border throughout its length. Total implant volume was 14ccs.
Using the 3D CT scan a custom jawline implant was designed that added some modest horizontal chin projection and jaw angle widths. But the greater augmentation effect by surface areas was along the entire jawline dropping down its inferior border throughout its length. Total implant volume was 14ccs.



 Under general anesthesia a submental incision was made combined with two intraoral posterior vestibular incisions. Through these incisions subperiosteal dissection was done on the sides and inferior border of the jawline. In doing so numerous chin and jaw angle ligaments needed to be released from the bone. Then the jawline implant was introduced through the submental incision and passed underneath the mental nerve and into position as per the design. Screw fixation was used at the chin and jaw angles.
Under general anesthesia a submental incision was made combined with two intraoral posterior vestibular incisions. Through these incisions subperiosteal dissection was done on the sides and inferior border of the jawline. In doing so numerous chin and jaw angle ligaments needed to be released from the bone. Then the jawline implant was introduced through the submental incision and passed underneath the mental nerve and into position as per the design. Screw fixation was used at the chin and jaw angles.

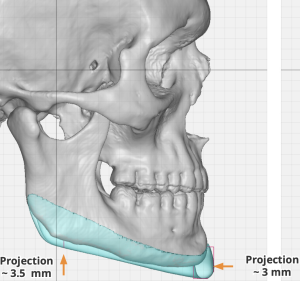
 While a vertical lengthening jawline implant can be designed, it has to be properly placed to exert its aesthetic effects. This requires doing a subperiosteal dissection along a jaw area where most surgeons are not used to dissecting…complete elevation of all soft tissues along the inferior border of the mandible. This becomes necessary when looking at the implant itself where a visible ledge is seen along the bottom of the implant. Getting this ledge, or the inferior edge of the implant, down over the bone is essential for implant placement. Getting good release along the harder to see inferior and posterior edge of the jaw angles is often the difference between good placement and implant malposition.
While a vertical lengthening jawline implant can be designed, it has to be properly placed to exert its aesthetic effects. This requires doing a subperiosteal dissection along a jaw area where most surgeons are not used to dissecting…complete elevation of all soft tissues along the inferior border of the mandible. This becomes necessary when looking at the implant itself where a visible ledge is seen along the bottom of the implant. Getting this ledge, or the inferior edge of the implant, down over the bone is essential for implant placement. Getting good release along the harder to see inferior and posterior edge of the jaw angles is often the difference between good placement and implant malposition.
Case Highlights:
1) In some vertically short faces the lower third of the jawline is the cause.
2) One method of elongating the lower face is a vertically lengthening implant that extends the entire inferior border of the jawline in a wraparound fashion from jaw angle to jaw angle.
3) The placement of a vertically lengthening custom jawline implant requires dissection along the entire inferior border, releasing specific osteocutaneous ligaments in doing so.
Dr. Barry Eppley
Indianapolis, Indiana