

Background: Otoplasty is the most common aesthetic ear surgery performed around the world. (not counting earlobe repair) While there are innumerable techniques by which it is performed the fundamental concept shared by all of them is a reshaping of the antihelical-helical rim cartilage shape. Sutures are the method by which the cartilage shape is maintained during surgery as well as in the early postoperative period until the cartilage memory is lost.
The application of sutures to bring back the protruding ear is not an exact science. The sutures are tightened to what the surgeon believes to be an acceptable ear shape. While the vast majority of time it is a major improvement under- or over correction is always possible. An overcorrected otoplasty is often called a telephone ear deformity because the ear now lies too close to the side of the head.
The presentation of a telephone ear deformity is variable. The hallmark of its existence is that the center of the ear is the most retruded part of the ear. This is seen as a ‘lost’ helical rim that now sits behind the anthelical rim. In some cases this is extreme and in others it can be quite subtle. But in the end it is the patient’s interpretation of its presence is what matters.

 Case Study: This male had a prior otoplasty years before which he felt was a bit overcorrected. The overcorrection was seen in the center third of the ear where the helical rim was at or just behind the anti helical rim. The direction of desired elevation of the helical rim was marked one each ear.
Case Study: This male had a prior otoplasty years before which he felt was a bit overcorrected. The overcorrection was seen in the center third of the ear where the helical rim was at or just behind the anti helical rim. The direction of desired elevation of the helical rim was marked one each ear.



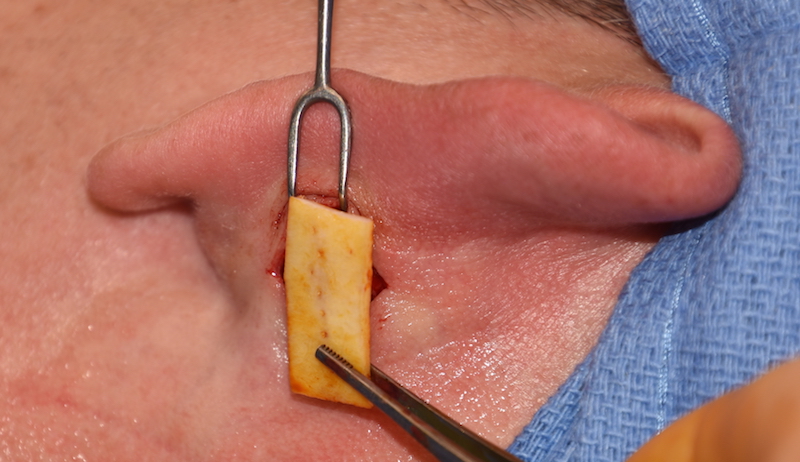
 Under local anesthesia a small postauricular incision was made in the crease. The ear cartilage was released from the deep temporal fascia out to the helical rim by removing all scar. Partial thickness cuts were made longitudinally in the cartilage. Tissue bank strips of rib cartilage were thawed and cut to length to fit into created pocket in a transverse orientation. This created a strut to hold the released ear cartilage more outward. The small incision was closed into layers and covered with a tissue glue for a dressing.
Under local anesthesia a small postauricular incision was made in the crease. The ear cartilage was released from the deep temporal fascia out to the helical rim by removing all scar. Partial thickness cuts were made longitudinally in the cartilage. Tissue bank strips of rib cartilage were thawed and cut to length to fit into created pocket in a transverse orientation. This created a strut to hold the released ear cartilage more outward. The small incision was closed into layers and covered with a tissue glue for a dressing.



 The immediate partial otoplasty reversal change could be seen. My observation has been that this changes little as the swelling subsides and the graft heals.
The immediate partial otoplasty reversal change could be seen. My observation has been that this changes little as the swelling subsides and the graft heals.
Trying to bring an ear back out, even for a small amount of change, requires structural support to do so. In essence it is a form of propping up the ear once it has been released. While a variety of materials and grafts can be used to do so the use of allogeneic or tissue bank rib cartilage offers an alternative that biologically lies somewhere between an implant and using the patient’s own cartilage. At the least it avoids a donor site harvest. But it does provide good structural support that is easily adaptable to the created postauricular tissue pocket.
Case Highlights:
1) The overcorrected otoplasty is typically seen by loss of view of the outer helical rim behind the anti helical fold in the central portion of the ear in the front view.
2) Postauricular release and vertical strut grafting with tissue bank rib cartilage brings the central helical rim put from behind the antihelical rim.
3) The cartilage graft is believed to incorporate into the natural ear cartilage through fibrous union long term.
Dr. Barry Eppley
Indianapolis, Indiana