


Background: One uncommon and not well known method of aesthetic jaw augmentation is a combined autologous-alloplastic approach. This combines the only aesthetic method of a jaw osteotomy with jaw implants. This means a bony genioplasty for the front of the jaw and custom implants for the back of the jaw.
The indication for this type of jaw augmentation is when a significant horizontal chin advancement is needed. While modest amounts of horizontal chin augmentation can be achieved by an implant there are limitations to what can be achieved with that approach. Because the soft tissue chin pad must be elevated off of the bone and if an implant is then placed on it, the soft tissue chin pad must be pulled back over it during closure. In the horizontal dimension this is not assured when large augmentations are desired. (10mms or greater) In my experience once 10mms or more of horizontal chin augmentation is needed it may be difficult or impossible on getting the soft tissue chin pad pulled back over it in a satisfactory manner. This can be overcome by a classic sliding genioplasty which does not have this soft tissue restriction as it naturally follows the bone forward due to its retained inferior soft tissue attachments.
With an autologous sliding genioplasty the jawline augmentation behind it can be done with implants. But it will require custom implant designs to create the desired jaw angle effect and have the implant come forward to blend into the relocated chin bone for a complete jawline augmentation.
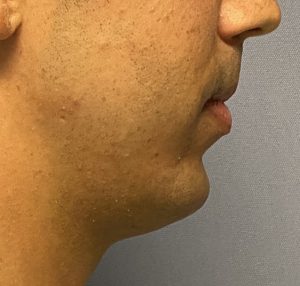
 Case Study: This young male sought a total lower jaw augmentation in which he had a combined horizontal chin deficiency with high jaw angles. His chin deficiency exceeded 10mms and it was also a bit long…or at least he didn’t want to to risk making it any longer. Because of his significant chin dimensional requirements a sliding genioplasty was planned for the chin and implants for the rest of his jawline.
Case Study: This young male sought a total lower jaw augmentation in which he had a combined horizontal chin deficiency with high jaw angles. His chin deficiency exceeded 10mms and it was also a bit long…or at least he didn’t want to to risk making it any longer. Because of his significant chin dimensional requirements a sliding genioplasty was planned for the chin and implants for the rest of his jawline.
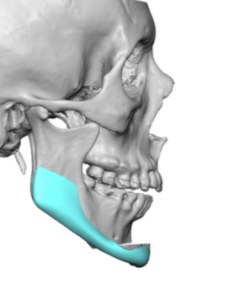
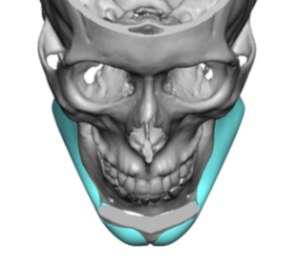 Using his 3D CT scan a horizontal movement sliding genioplasty was planned of 12mms with a vertical shortening of 2mms. Custom extended jawline implants were designed for the rest of the jaw augmentation which principally provided some vertical length and linearity to the jawline behind the chin. They merged with the sliding genioplasty by crossing the back ends of the chin osteotomies and along the advanced chin almost to the midline.
Using his 3D CT scan a horizontal movement sliding genioplasty was planned of 12mms with a vertical shortening of 2mms. Custom extended jawline implants were designed for the rest of the jaw augmentation which principally provided some vertical length and linearity to the jawline behind the chin. They merged with the sliding genioplasty by crossing the back ends of the chin osteotomies and along the advanced chin almost to the midline.



 Under general anesthesia this combined autologous-implant jaw augmentation procedure done together initially setting the sliding genioplasty position first. Then using posterior vestibular mucosal incisions the implant pocket for the rest of the was developed and also served as entry site for the implants. One of the key intraoperative maneuvers is to get the anterior extensions of the implants onto the front end of the chin bone in proper position after the jaw angle portion of the implants was positioned and secured with screws.
Under general anesthesia this combined autologous-implant jaw augmentation procedure done together initially setting the sliding genioplasty position first. Then using posterior vestibular mucosal incisions the implant pocket for the rest of the was developed and also served as entry site for the implants. One of the key intraoperative maneuvers is to get the anterior extensions of the implants onto the front end of the chin bone in proper position after the jaw angle portion of the implants was positioned and secured with screws.
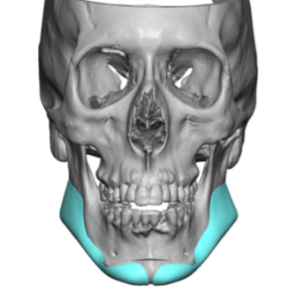 When designing the implants for this combined bony-implant jaw augmentation procedure, the anterior extensions must come way forward and significantly onto the chin. One can choose to shorten the during surgery if desired but you can’t make the longer if they are too short. One needs a greater extension onto the chin than it may appear in the implant design so that it can be secured with a single screw per side.
When designing the implants for this combined bony-implant jaw augmentation procedure, the anterior extensions must come way forward and significantly onto the chin. One can choose to shorten the during surgery if desired but you can’t make the longer if they are too short. One needs a greater extension onto the chin than it may appear in the implant design so that it can be secured with a single screw per side.
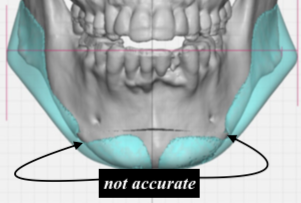 Unlike using this combined approach for a vertical chin lengthening osteotomy, the forward moving sliding genioplasty will create bony wings out to the side on their back part. The surgeon needs to be aware that this may will make for some challenges in getting the implant around it. The protruding wing is never accurately shown in computer diagrams but it is almost always there.
Unlike using this combined approach for a vertical chin lengthening osteotomy, the forward moving sliding genioplasty will create bony wings out to the side on their back part. The surgeon needs to be aware that this may will make for some challenges in getting the implant around it. The protruding wing is never accurately shown in computer diagrams but it is almost always there.
Case Highlights:
1) Significant horizontal lengthening of the chin is best done by a sliding genioplasty anteriorly and using custom implants to complete the lower jaw augmentation.
2) Preoperative computer designing is needed to make the repositioned chin bone and implant fit together for a unified jawline look.
3) While computer designing makes it look easy to put the two jaw augmentation concepts together, in actual surgery it is always a bit more difficult than it diagrammatically appears.
Dr. Barry Eppley
Indianapolis, Indiana