

Background: A large Adam’s apple or thyroid cartilage causes a visible prominence in the contour of the neck. This is a common feature of many male necks and thus is not seen as aesthetically undesirable unless it is extremely large. In contrast females prefer a smoother neck contour with little to no thyroid cartilage prominence. These gender aesthetic preferences explain the frequency of tracheal reductions done in facial feminization surgery particularly in transfemales.
In tracheal shave surgery the pertinent issues are where is the incision location, the method of cartilage reduction to be used, should the location of the vocal cords be established before performing the reduction and how much cartilage should be removed.
The answers to which are…Multiple incision locations over or near the thyroid cartilage have been used. But the cervicomental incision just above the thyroid cartilage works best for most patients. As a safety measure it is hard to argue that endoscopic visualization of the vocal cords should not be done before the cartilage reduction is started.The amount of cartilage reduction should be to the point of some instability between the two thyroid cartilage halfs. The scalpel is the most controlled way to shave the prominent cartilages down provided they are still soft.and easily carvable. Once they get stiffer/partially calcified and one is below the thyroid notch than a high speed hand-piece and burr is needed.
Case Study: This female patient had a very prominent Adam’s apple that had a near 90 degree angle at the anterior edges of the thyroid notch/laryngeal incisure.

 Under general endotracheal anesthesia a cervicomental skin incision was made and the thyroid cartilage exposed. The location of the vocal cords was seen and marked with a 25 gauge needle insertion.
Under general endotracheal anesthesia a cervicomental skin incision was made and the thyroid cartilage exposed. The location of the vocal cords was seen and marked with a 25 gauge needle insertion.

 With the cartilage exposure a very asymmetric midline position was seen between the two thyroid plate halves. A scalpel was then used to shave down the greatest cartilage prominences until the mobility between the two paired cartilage segments was acceptably ‘unstable’.
With the cartilage exposure a very asymmetric midline position was seen between the two thyroid plate halves. A scalpel was then used to shave down the greatest cartilage prominences until the mobility between the two paired cartilage segments was acceptably ‘unstable’.
 The strap muscles were closed over the cartilages and the small skin incision closed with very small dissolvable sutures.
The strap muscles were closed over the cartilages and the small skin incision closed with very small dissolvable sutures.
![]()
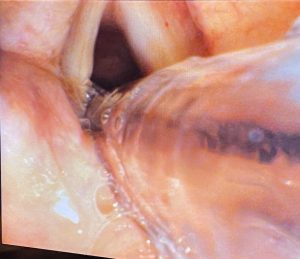
![]() The reduction in the thyroid cartilages could be appreciated intraoperatively.
The reduction in the thyroid cartilages could be appreciated intraoperatively.
The greatest projection of the prominent Adam’s apple is at the central thyroid notch. As this area is reduced the base plate of the thyoid cartilages are encountered which become stiffer and less successfully reduced by a scalpel. As the anterior attachments of the vocal cords are typically below the thyroid notch cartilage reduction below the notch area pose the greatest risk of injury.
Key Points:
1) The cervicomental incision offer a less visible incision site but still with good access to the thyroid cartilages.
2) Intraoperative endoscopic visualization of the vocal cords before and after thyroid cartilage reduction provides an additional safety measure.
3) One reason for thyroid cartilage prominence is an asymmetry between the two halves with a larger more prominent side.
Dr. Barry Eppley
World-Renowned Plastic Surgeon