

Background: Facial asymmetries are not uncommon and can affect any of the facial thirds.Such asymmetries can be more complete affecting multiple facial thirds or they can only involve one of them. The upper facial third or forehead is not spared from such congenital asymmetries although in my experience it is probably less commonly affected than the lower two thirds of the face. But it does occur it can be very noticeable due to the large surface area of the forehead.
There is wide variability to forehead asymmetries depending on what part of the forehead anatomy is affected. The most common forehead asymmetry is unilateral and affects the bony temporal line. This line represents the side of the forehead and is the transition between the anterior bony forehead and the lateral muscular temporal area. Depending upon its severity it can affect part or all of the bony temporal line. For example, in plagiocephaly, the entire temporal line is affected with a forward protrusion on the affected side.
But depressed or recessed deformities of the temporal line is more common. Most commonly the temporal line or upper side of the forehead is recessed which usually does not involve the tail of the brow bone. More rarely the lower end of the temporal line or tail of the brow bone can be affected in isolation. This probably occurs due to in utero compression. When the brow bone is affected it can be one of the visible forehead asymmetries due to its proximity to the eyes.
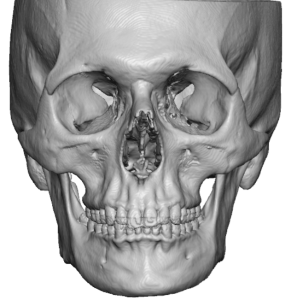
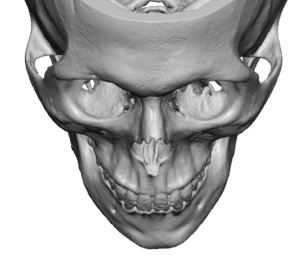 Case Study: This male has an isolated forehead asymmetry affecting the right tail of the brow bone. His 3D CT scan showed a recession of the right tail of the brow bone down to the frontozygomatic suture line. It extended superiorly only up through the suprabrow bone break.
Case Study: This male has an isolated forehead asymmetry affecting the right tail of the brow bone. His 3D CT scan showed a recession of the right tail of the brow bone down to the frontozygomatic suture line. It extended superiorly only up through the suprabrow bone break.
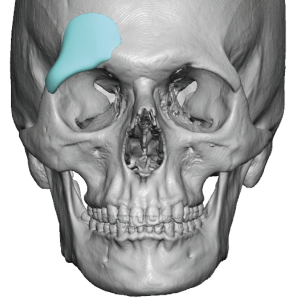
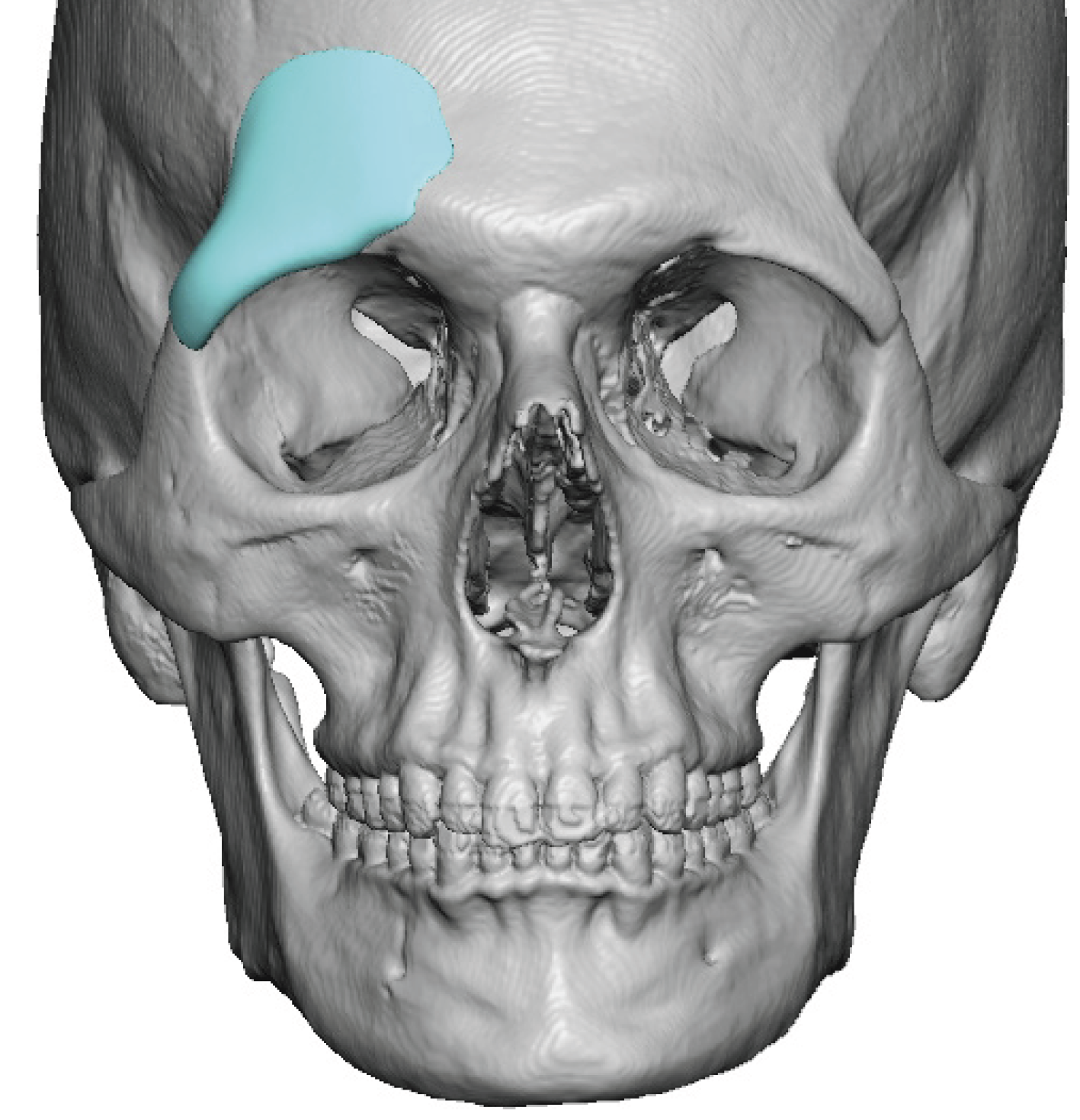
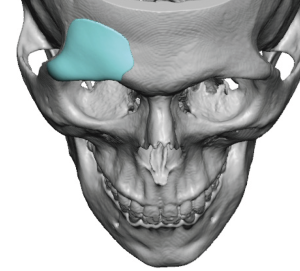 A custom brow bone implant was designed based on mirroring the shape of the opposite normal left brow bone. Its maximum thickness was 2.8mms with a total implant volume of 2.2ccs.
A custom brow bone implant was designed based on mirroring the shape of the opposite normal left brow bone. Its maximum thickness was 2.8mms with a total implant volume of 2.2ccs.
 Due to its small size and the location over the tail of the brow bone an upper eyelid incision was used for implant placement. This allows for direct access for any lateral brow bone procedure or unilateral lower forehead procedure. Adequate tail of the brow bone subperiosteal release can then be done under direct vision.
Due to its small size and the location over the tail of the brow bone an upper eyelid incision was used for implant placement. This allows for direct access for any lateral brow bone procedure or unilateral lower forehead procedure. Adequate tail of the brow bone subperiosteal release can then be done under direct vision.

 Through the eyelid incision the brow bone implant was inserted, positioned and secured with a single microscrew.
Through the eyelid incision the brow bone implant was inserted, positioned and secured with a single microscrew.
 The upper eyelid incision was then closed with small 6-0 plain sutures for what would eventually become an invisible scar line.
The upper eyelid incision was then closed with small 6-0 plain sutures for what would eventually become an invisible scar line.

 The immediate effects of the brow bone asymmetry correction couold be appreciated intraoperatively.
The immediate effects of the brow bone asymmetry correction couold be appreciated intraoperatively.
It is tempting to look at a small bony deficiency and just treat it by an ‘eyeball’ approach making a handmade implant intraoperatively. While this is not a wrong approach at best it would lessen the size of the defect (undersized implant) or at worse create a different form of asymmetry. (over sized implant) The eye is simply not precise enough to create the most ideal correction. This is the benefit of a custom implant design using the patient’s 3D CT scan and ask the program to match the bone shapoe/projection on the normal side.
Key Points
1) Bony forehead asymmetries of congenital origin can be either high (upper forehead) or low (brow one area).
2) A custom implant design is the most accurate method for reconstruction of forehead and brow bone asymmetries.
3) For brow bone asymmetries an upper eyelid incisional approach can be used for the custom brow bone implant placement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon