


Background: The treatment of the protruding ear is a common and historic plastic surgery procedure. While various techniques exist to pull back the concha cartilage and /or create a more defined anti helical fold to reduce the auriculocephalic angle their effects are primarily at the middle third of the ear. In such setback otoplasties the upper third of the ear usually moves inward as well with the ear cartilage manipulations below it.
For a few patients they may found after traditional setback otoplasty surgery that they wish the upper part of the ear was closer to the side of the head. There are also patients with otherwise normal positioned ears in which it is only the upper part of the ear which is protrusive. This is particularly seen in men who have very short cut hair for shave their heads ins which they see the upper easier as protrusive.
In these isolated protruding upper ears traditional setback otoplasty techniques will not be effective. Bending the scapha cartilage by sutures will only crimp and deform the upper ear. A different setback method is needed.
Case Study: This male had a normal ear shape and position on the side of his head with the exception of the top of the ear that protruded laterally. He had a well defined antihelical fold and his concha-mastoid angle was normal.

 Under general anesthesia (although it could also be done under local) the upper postauricular sulcus excision site was marked. More skin removal was marked on the ear side than the side of the head. Full thickness skin was excision along the edges of the markings to expose the ear cartilage and the deep temporal fascia.
Under general anesthesia (although it could also be done under local) the upper postauricular sulcus excision site was marked. More skin removal was marked on the ear side than the side of the head. Full thickness skin was excision along the edges of the markings to expose the ear cartilage and the deep temporal fascia.

 Slowly resorbing sutures were placed between the scapha of the upper ear and the deep temporal fascia pulling the upper ear tight against the side of the head.The skin edges were closed with rapidly dissolving dermal and skin sutures. The remaining open part of the upper ear skin was glued to the side of the head so no external wrap dressing was needed.
Slowly resorbing sutures were placed between the scapha of the upper ear and the deep temporal fascia pulling the upper ear tight against the side of the head.The skin edges were closed with rapidly dissolving dermal and skin sutures. The remaining open part of the upper ear skin was glued to the side of the head so no external wrap dressing was needed.
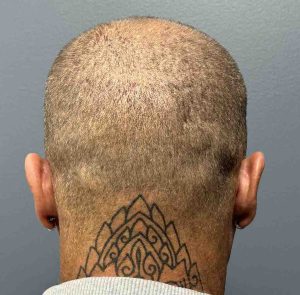
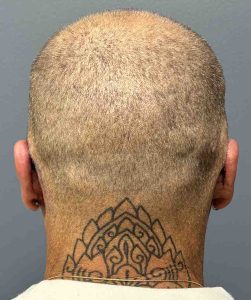
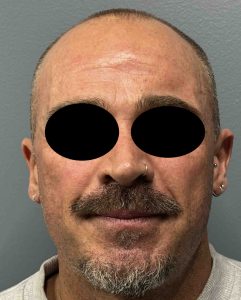
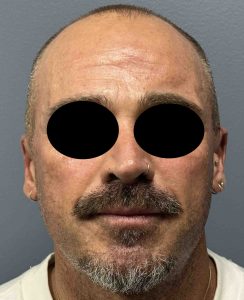 When seen the next day the maximal setback of the upper ears could be seen in both the back and frontal views..
When seen the next day the maximal setback of the upper ears could be seen in both the back and frontal views..
The upper ear setback requires a novel technique to do so since it does not depend on reshaping of the ear cartilages. Rather it requires moving the upper ear closer to the side of the by suturing it to the temporal fascia. This requires that the skin on both sides of the sulcus be partially removed to allow a pathway for the suture placement. Besides the sutures the long term stability of the setback is aided by the reduction in the depth of the sulcus.
What is important to point out is that this is an immediate result and the top of the ears have been deliberately glued to the side of the head for early support. This glue will eventually separate and the residual reduced sulcus depth will be seen. This will result in some ‘relapse’ ,although it is not really relapse, with a less than glued to the side of the head upper ear appearance. It will take some time to see the true final result with the effects of swelling resolution and then healing and scar contracture.. How much retained permanent inward positioning of the top of the ear remains to be seen although there is always in my experience less what existed preoperatively. There is a more aggressive technique in which the postauricular sulcus is completely eliminated which then makes it look like a glued to the side of the head appearance. But before jumping to that potentially unatural appearance and having no sulcus at all the subtotal sulcus reduction approach is the safest initial approach. One can always graduate to complete sulcus elimination if the patient is certain that the subtotal sulcus reduction is not enough of a result.
Key Points:
1) Setback otoplasties are based on concha and antihelical fold cartilage reshaping techniques.
2) Setback of the protruding upper 1/3 of the ear requires changes in the postauricular sulcus to allow for cartilage to fascia suturing.
3) This sulcus reduction technique pulls the top of the ear closer to the side of the head with loss of sulcus depth.
Dr. Barry Eppley
World-Renowned Plastic Surgeon