

Background: While facial feminization surgery (FFS) is now a recognized niche area of plastic surgery its counterpart, facial masculinization surgery (FMS) ,is less well known. While it has long been done in a limited fashion with some standard procedures. (e.g., chin augmentation) other procedures to specifically masculinize the face are less frequently performed or are most surgeons even aware that they exist.
While facial feminization surgery procedures are largely reductive in nature facial masculinization procedures revolve around augmentation. This means that implants are almost always needed to masculinize the face to create a more defined and/or angular appearance.This can be done at all three levels of the face with the jawline usually being the most requested change for many patients. After the jawline the upper third of the face (forehead-brow region) has the most significant masculinizing effect.
It is well known that one of the major differences between masculine and feminine faces is in the upper third of the face. The male face develops a larger and more projecting frontal sinus area as well as more protuberant superior orbit. Other features of a masculine upper face include a longer forehead which is also broader and flatter. In addition, the male globe position is relatively recessed with a relatively smaller orbit compared to females.
As there are no standard forehead or brow bone implants, the only effective method mis a custom forehead-brow bone implant.
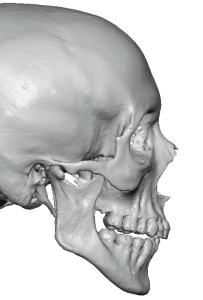
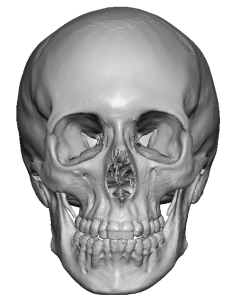 Case Study: This young patient desired a more masculine appearance and felt that the upper third of the face was the most important change needed. The 3D CT scan show minimal brow bone development and a rounder and more recessed slope of the forehead. The goal was for a modest but not a dramatic change.
Case Study: This young patient desired a more masculine appearance and felt that the upper third of the face was the most important change needed. The 3D CT scan show minimal brow bone development and a rounder and more recessed slope of the forehead. The goal was for a modest but not a dramatic change.

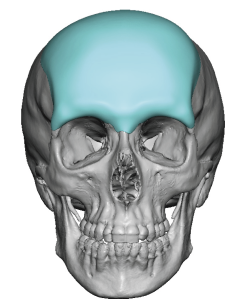 A custom forehead-brow bone implant was designed that provided 5mms of brow bone and 4mms of forehead projection. The implant design also improved the backward slope of the forehead by extending back across the top of the head.
A custom forehead-brow bone implant was designed that provided 5mms of brow bone and 4mms of forehead projection. The implant design also improved the backward slope of the forehead by extending back across the top of the head.

 Under general anesthesia and through a small superior scalp incision a subperiosteal pocket was developed with full release of the tissues across the brow bones from one frontozygomatic suture line to the other.
Under general anesthesia and through a small superior scalp incision a subperiosteal pocket was developed with full release of the tissues across the brow bones from one frontozygomatic suture line to the other.
 Once in good position it was secured by two small microscrews to the skull to keep it adequately positioned low enough over the brows.
Once in good position it was secured by two small microscrews to the skull to keep it adequately positioned low enough over the brows.

 The four month postoperative results showed the desired augmentative change in the shape of the upper face.
The four month postoperative results showed the desired augmentative change in the shape of the upper face.
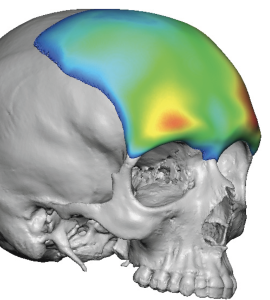 Augmentation of the forehead is the largest area of the face that can be done by surface area coverage. By definition every forehead augmentation must extend behind the frontal hairline so technically it involves skull coverage as well. The key to such an implant design to have a more natural looking result is that surface area coverage is more important that any one ares of thickness. Not that various thicknesses are not important just that they have to be incorporated in a large enough implant base so they blend in naturally.
Augmentation of the forehead is the largest area of the face that can be done by surface area coverage. By definition every forehead augmentation must extend behind the frontal hairline so technically it involves skull coverage as well. The key to such an implant design to have a more natural looking result is that surface area coverage is more important that any one ares of thickness. Not that various thicknesses are not important just that they have to be incorporated in a large enough implant base so they blend in naturally.
Case Highlights:
1) Masculinizing the upper third of the face requires a custom forehead implant that incorporates the lower brow bones.
2) In designing a custom forehead implant considerations must be given to how much brow bone projection is desired along with how much forehead slop correction is needed.
3) A large custom forehead-brow bone implant can be placed through a remarkably small scalp incision in comparison to the size of the implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon