


Background: Lip augmentation is one of the most common female facial enhancements. It is by far most commonly done by injection methods whether it is by synthetic fillers or fat. The success of such volume addition is dependent on how much vermilion show is present. If the vermilion is height is small or vertically short the added volume pushes out and not up creating the classic duck lip effect.
This is exactly what occurs in the so called ‘pencil’ upper lip. Not to be confused with a lip pencil the pencil lip refers to a lip shape with very limited vermilion show. This typically affects the upper lip with scant vermilion show from mouth corner to mouth corner. There is also a flatter cupid’s bow shape with inconspicuous philtral peaks. There is a very visible upper and lower lip vermilion disproportion.
While injectable fillers are often tried in the pencil upper lip they are in effective at improving the vermilion disproportion. They are better treated by surgical lip procedures. The most common surgical approach would be a subnasal lip lift but this only affects the central part of the lip and even then its effect would be limited and incomplete across the full horizontal length of the lip. This is where the vermilion advancement procedure is most indicated. But how much to elevate the whole upper lip vermilion is partially affected by the length of the upper lip. Usually the pencil shaped upper lip is also too long. But in some cases may be very short as well.
 Case Study: This female desired to have a more visible upper lip size. She had a very thin upper lip with minimal cupid’sbow shape. There was a center
Case Study: This female desired to have a more visible upper lip size. She had a very thin upper lip with minimal cupid’sbow shape. There was a center
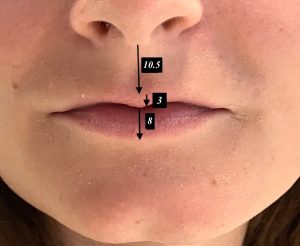 It had a 3mm vertical vermilion height compared to an 8mm lower lip vermilion height. Her upper lip length was modestly short at 10.5mms.
It had a 3mm vertical vermilion height compared to an 8mm lower lip vermilion height. Her upper lip length was modestly short at 10.5mms.
 While it may be ideal to have an upper lip advancement that would equal the height of the lower lip (5mm advancement) the upper lip was too short to permit that much vermilion height change. Instead a 3mm advancement was marked which would not exactly match the upper lip size to that of the lower lip. Given the limited cupid’s bow shape its limited shape was maintained with the advancement so it did not look unnatural.
While it may be ideal to have an upper lip advancement that would equal the height of the lower lip (5mm advancement) the upper lip was too short to permit that much vermilion height change. Instead a 3mm advancement was marked which would not exactly match the upper lip size to that of the lower lip. Given the limited cupid’s bow shape its limited shape was maintained with the advancement so it did not look unnatural.
 Under general anesthesia as other procedures were being done, the final procedure was the upper lip advancement. The intervening skin was excised and the vermilion advanced and closed with 6-0 Vicryl as the deeper layer and 6-0 plain for the outer closure.
Under general anesthesia as other procedures were being done, the final procedure was the upper lip advancement. The intervening skin was excised and the vermilion advanced and closed with 6-0 Vicryl as the deeper layer and 6-0 plain for the outer closure.
Key Points:
1) For very thin upper lips the most effective augmentation strategy is a vermilion advancement.
2) In thin upper lips that have a short nose-lip distance a conservative upper lip advancement is advised.
3) Like all surgical lip enhancement procedures precision in the markings and execution is needed to avoid lip asymmetries.
Dr. Barry Eppley
World-Renowned Plastic Surgeon