

Background: V line surgery is a well known technique for lower jaw reduction/narrowing. In its most recognized form it is a full thickness bony removal through the jaw angles tapering to an end in the mid-body of the mandible. It is often combined with a separate chin procedure to continue the narrowing effect usually through a modified sliding genioplasty which changes the length of the chin as well as narrows it. The procedure has its origins in Asian patients who are more prone to wide and pronounced jaw angles and is most commonly performed jn this part of the world die to greater patient need.
While this radical bone removal through the jaw angles is very effective at narrowing the jawline, as particularly seen in the frontal view, it has its aesthetic tradeoffs. One of these tradeoffs is the potential risk of soft tissue sagging with the loss of bone support from the reduced jaw angles. When this occurs the only treatment is some form of jowl tuck lower facelift procedure, which while effective, is a procedure that the typical young female patient who has this procedure would like to avoid.
As a V line alternative to traditional amputation of the jaw angles is decortication. By removal of the outer cortical layer of the jaw angles, but leaving its shape intact (the very point of the jaw angles can be fully removed), jaw angle width is reduced. It is not reduced as much as with traditional V line surgery because that has a bicortical effect. But by preserving one of the critical layers the risk of soft tissue sagging is eliminated and the masseteric muscle sling remains intact.
Case Study: This young Asian female had a prior chin implant surgery to provide increased horizontal projection but to also make the chin more narrow. A modified anatomic chin implant was placed higher up on the chin bone to prevent the chin from becoming vertically longer. (In essence an implant form of mini V line surgery)

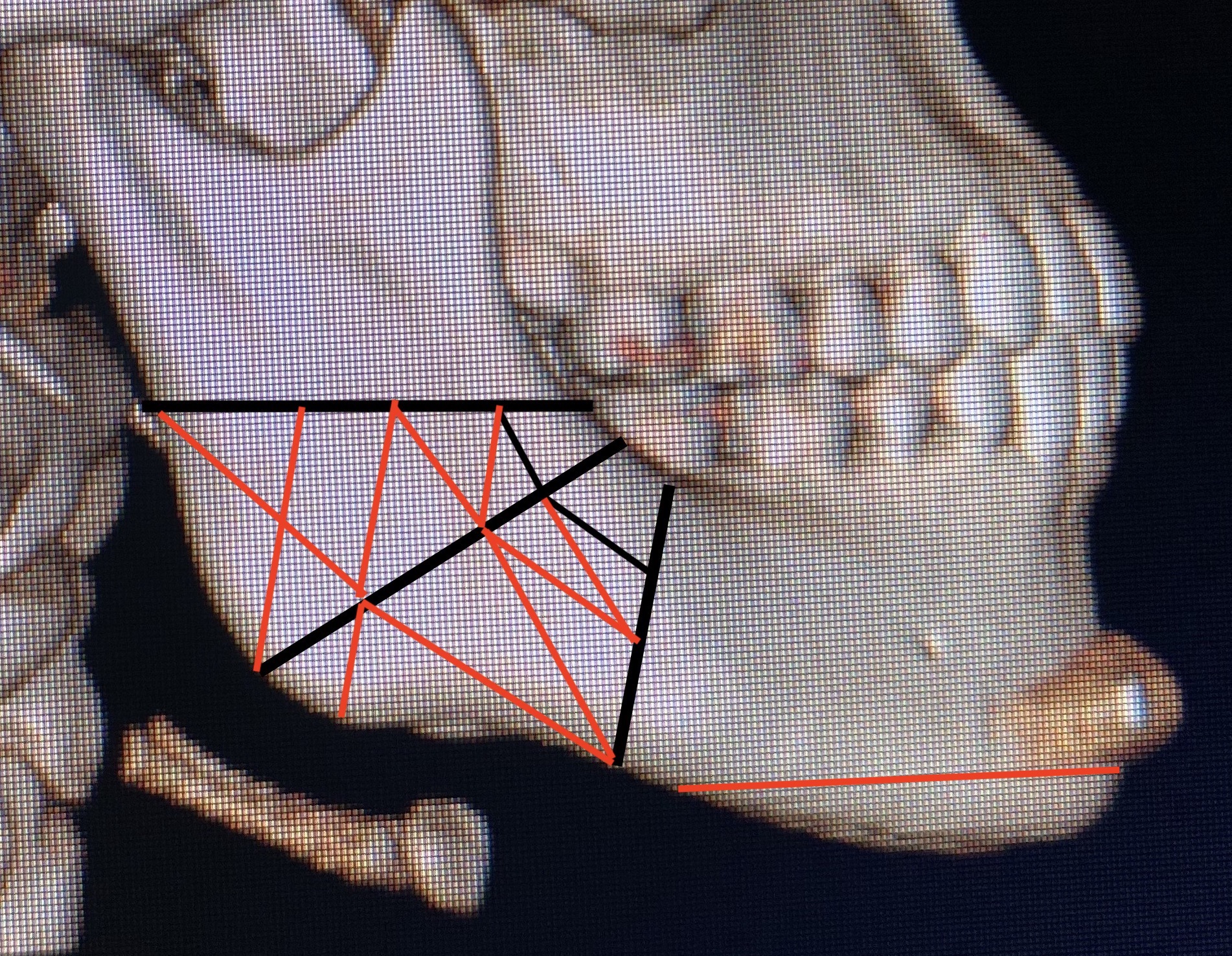
 She now desired for the rest of her jawline to be made smaller/reduced but feared soft tissue sagging. Thus her surgical plan consisted of jaw angle reduction by decortication (keeping its shape but reducing its thickness) using initial saw cuts through the outer cortex to mark the depth of the bone removal with burring reduction between them and anterior to the vertical cut onto the body of the mandible. This was to be combined with an inferior border shave of the anterior half of the jawline using her existing submental scar.
She now desired for the rest of her jawline to be made smaller/reduced but feared soft tissue sagging. Thus her surgical plan consisted of jaw angle reduction by decortication (keeping its shape but reducing its thickness) using initial saw cuts through the outer cortex to mark the depth of the bone removal with burring reduction between them and anterior to the vertical cut onto the body of the mandible. This was to be combined with an inferior border shave of the anterior half of the jawline using her existing submental scar.

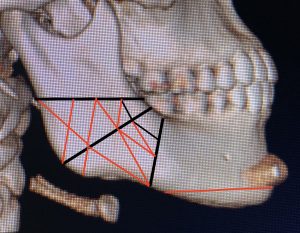
 Under general anesthesia and through posterior vestibular incisions the jaw angle width reductions were performed by saw cuts and bone burring as per the diagram.
Under general anesthesia and through posterior vestibular incisions the jaw angle width reductions were performed by saw cuts and bone burring as per the diagram.





 Then through the existing submental scar the inferior border shave was done up to the lower level of the chin implant with bilateral full thickness bone cuts. The U-shaped inferior border segment was split in the middle for removal. To make the submental soft tissue match the elevated chin-jawline the geniohyoid muscle was resuspended to the level of the chin bone and the submental region was directly defatted prior to closure.
Then through the existing submental scar the inferior border shave was done up to the lower level of the chin implant with bilateral full thickness bone cuts. The U-shaped inferior border segment was split in the middle for removal. To make the submental soft tissue match the elevated chin-jawline the geniohyoid muscle was resuspended to the level of the chin bone and the submental region was directly defatted prior to closure.
 As a final lower facial reshaping procedure perioral liposuction was performed on both sides for reductive contouring above the jawline.
As a final lower facial reshaping procedure perioral liposuction was performed on both sides for reductive contouring above the jawline.
In this V line jaw reduction surgery variation multiple different approaches were taken to achieve a lower facial narrowing that did not risk soft tissue sagging and took advantage of a prior chin implant placement. The most applicable part of this case study is how to reduce jaw angle widths without losing soft tissue support. This is not a technique for many V line surgery patients who have really strong and prominent jaw angles/lower jaws where full thickness bone removal of the jaw angles is needed to get a significant improvement. (and the risk of soft tissue sagging may be worth it) But in patients who have ‘normal’ jaw angles or even higher jaw angles decortication is the safer aesthetic technique that does not risk over correction and/or soft tissue sagging.
Case Highlights:
1) Westernized jaw reduction refers to reducing jaw angle width but preserving its shape in an effort to prevent postoperative soft tissue sagging.
2) Decortication of the outer bone layer of the jaw angles is done through a combination of saw cuts and bone shaving.
3) The chin and anterior jawline can be vertically reduced by an inferior border shave technique.
Dr. Barry Eppley
Indianapolis, Indiana