

The newest member of the body implant family is that of hip implants. Augmentation of the lower torso has been done by various styles of buttock implants for decades. While the majority of buttock augmentation today is done by fat injections (aka Brazilian butt lift), there has been a relative neglect of the hips to the side of the buttocks due to either a lack of adequate fat to inject them or poor fat graft take over the often concave and tighter tissues of the trochanteric hip region.
From an anatomic standpoint, the hip augmentation zone extends from below the superior iliac crest down over the trochanteric tuberosity of the femur bone. Underneath the skin and fat layers lies the tensor fascia late muscle/fascia (TFL) which attaches to the iliac crest and runs continuous with the iliotibial band (ITB) down to the side of the knee where it attaches to the lateral epicondyle. At its superior extent the TFL combines with the posterior ITB to create the upper half of the hip fascia. Posteriorly this thick fascia connects to the gluteus maximus muscle creating an overall continuous sheet. Underneath the ITB inferiorly is the vastus laterals muscle. The function of the TFL is for hip movement specifically abduction, flexion and internal rotation.
 When considering alloplastic hip augmentation one has to decide whether it is to be placed above or below the TFL. This is primarily determined by the size of the implant and the desired dimensions of hip augmentation. Subfascial placement of the implant is more restrictive in size and will have some short term functional issues. (short term side of the knee discomfort due to the ITB attachment It is somewhat analogous to intramuscular buttock implants where the size of the implant is also restricted and it will induce temporary limited range of motion. When the hip augmentation needs are not excessive a subfascial pocket location can be effective and falls into the general implant philosophy that the tissue coverage an implant has the better.
When considering alloplastic hip augmentation one has to decide whether it is to be placed above or below the TFL. This is primarily determined by the size of the implant and the desired dimensions of hip augmentation. Subfascial placement of the implant is more restrictive in size and will have some short term functional issues. (short term side of the knee discomfort due to the ITB attachment It is somewhat analogous to intramuscular buttock implants where the size of the implant is also restricted and it will induce temporary limited range of motion. When the hip augmentation needs are not excessive a subfascial pocket location can be effective and falls into the general implant philosophy that the tissue coverage an implant has the better.
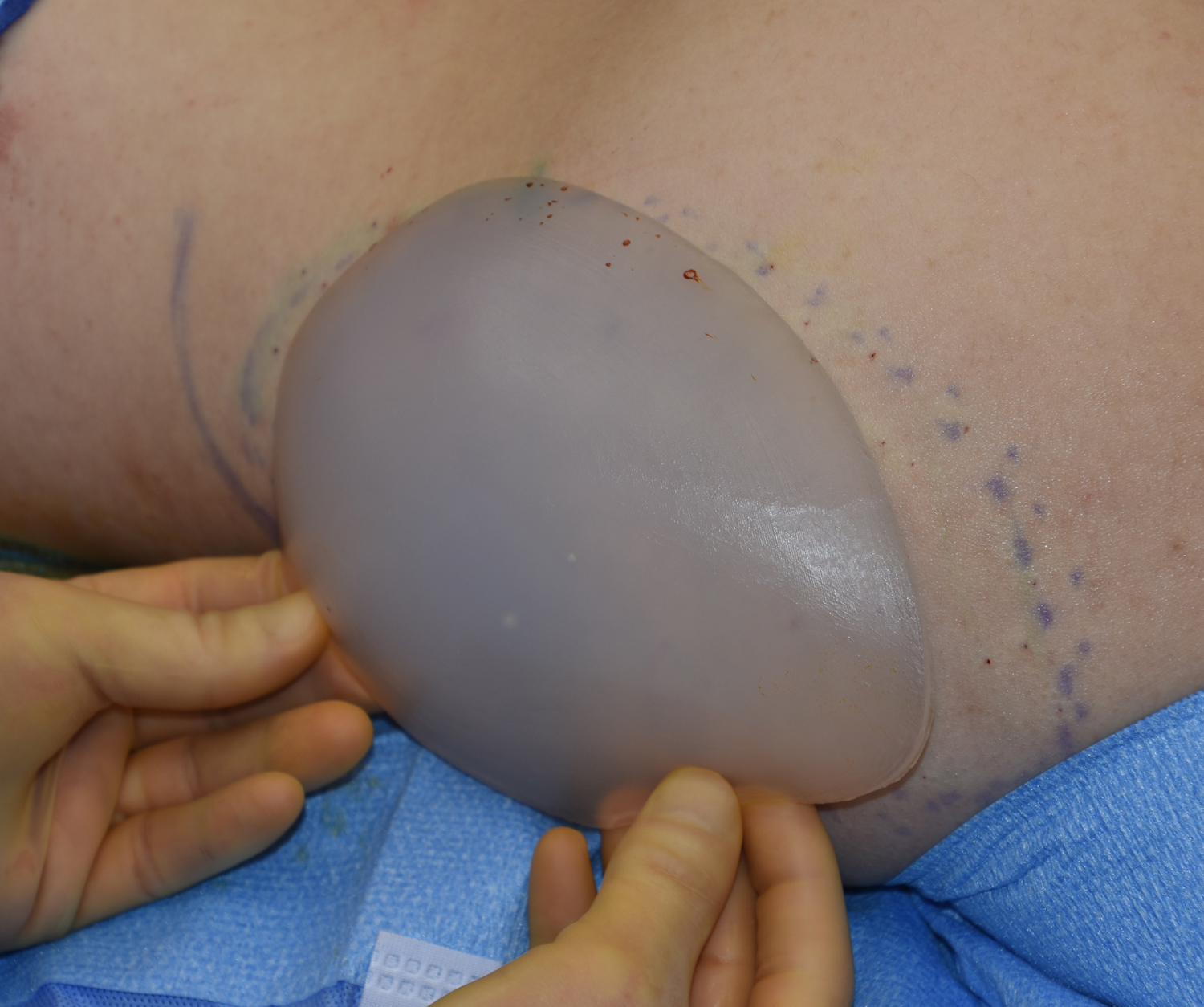
 On top of the fascia or a deep subcutaneous pocket location in hip augmentation offers the opportunity for larger implants both in perimeter surface area of coverage but also in thickness. Having placed numerous such hip implants I have observed that the thickness of the implant is less important than how much surface area it covers. Greater surface area coverage also allows for a smoother transition into the surrounding buttock and thigh contours. Broader hip implants also requires that their softness (durometer) be the lowest possible so they do not feel restrictive in any way.
On top of the fascia or a deep subcutaneous pocket location in hip augmentation offers the opportunity for larger implants both in perimeter surface area of coverage but also in thickness. Having placed numerous such hip implants I have observed that the thickness of the implant is less important than how much surface area it covers. Greater surface area coverage also allows for a smoother transition into the surrounding buttock and thigh contours. Broader hip implants also requires that their softness (durometer) be the lowest possible so they do not feel restrictive in any way.
Hip augmentation can be successfully done using implants. Currently there are no standard sizes or styles of these body implants. Currently I make all such implants are a custom basis based on patient measurements of surface area coverage.
Dr. Barry Eppley
Indianapolis, Indiana