


Rib 11–12 vs Rib 10–12 Resection
Advanced Waist Contouring — Indications, Impact, and Risk Escalation
This comparison applies to advanced, carefully selected aesthetic cases. Rib 10 involvement changes the operation from flank refinement to structural waist narrowing.
1. Anatomical Importance
Ribs 11–12
- Both are floating ribs
- Influence the lower third of the waist
- No role in chest wall stability
Effect zone
- Lower flank
- Back and rear oblique views
Ribs 10–12
 Rib 10 is a false rib loosely attached to the costal margin via cartilage
Rib 10 is a false rib loosely attached to the costal margin via cartilage- Major contributor to true waist width along with rib 11
- Still has a significant downward inclination but turns horizontally at its anterior costal attachment
- Functionally integrated with:
- External oblique
- Costal margin stability
- Upper abdominal wall
 Rib 10 is a false rib loosely attached to the costal margin via cartilage
Rib 10 is a false rib loosely attached to the costal margin via cartilage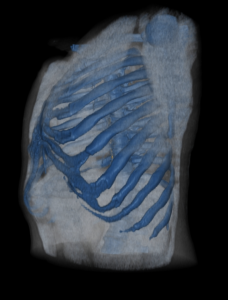 Still has a significant downward inclination but turns horizontally at its anterior costal attachment
Still has a significant downward inclination but turns horizontally at its anterior costal attachmentEffect zone
- Entire waist cylinder
- Frontal, oblique, and back views
2. Visual Contour Difference
|
Feature |
Rib 11–12 |
Rib 10–12 |
|
Lower flank smoothing |
?????? |
?????? |
|
True waist narrowing |
???? |
???????? |
|
Frontal silhouette |
Mild–moderate |
Moderate–significant |
|
Ribcage width change |
Minimal |
Definite |
|
“Hourglass” effect |
Limited |
Achievable in select patients |
Key distinction
- Rib 11–12 reshapes the lower waist
- Rib 10–12 reshapes the rib cage itself
3. Surgical Complexity & Risk
Rib 11–12 (Type 1)
- Posterolateral or wavy vertical incisional approach
- LD muscle-splitting for access
- Low risk of encountering lung pleura
Rib 10–12 (Type 2)
- Wider thicker rib
- Is more stiff once mobilized due to the anterior subcostal attachments
- Higher likelihood of encountering the lung pleura on the backside of the rib
- Can be treated by three different methods: partial resection (out to anterior costal attachment), limited resection (bridge collapse technique) and segmental resection and shortening with plate fixation
- Allows for greater latissimus dorsi muscle resection/plication
 Wider thicker rib
Wider thicker rib Can be treated by three different methods: partial resection (out to anterior costal attachment), limited resection (bridge collapse technique) and segmental resection and shortening with plate fixation
Can be treated by three different methods: partial resection (out to anterior costal attachment), limited resection (bridge collapse technique) and segmental resection and shortening with plate fixation4. Functional Considerations
11–12
- No measurable impact on respiration
- Oblique strength preserved
10–12
- Temporary reduction in core comfort
- Long-term function typically normal
5. Patient Selection (Critical)
Appropriate for Rib 11–12
- Boxy lower waist
- Long floating ribs
- First-time rib contouring
- Patient interested in more ‘limited’ surgery
Appropriate for Rib 10–12
- Very wide or flared lower rib cage
- Short-waisted torso
- Athletic / low-BMI patients
- Interested in maximal waist reduction approach
- Revision cases with inadequate narrowing
Not ideal for rib 10–12
- Thick subcutaneous fat
- Loose skin
- Unrealistic expectations
- Desire for “corset-like” effect
6. Combination Strategy
Rib 10–12 cases almost always require:
- High-definition flank lipo
- Careful symmetry control
- Conservative bilateral planning
Lipo without rib 10 removal cannot substitute for rib cage narrowing.
7. Rib Removal Concepts
- Rib 11–12:
“Reshaping the lower waist without changing the rib cage.” - Rib 10–12:
“Actual narrowing of the lower rib cage”
Bottom-Line Rib Removal Surgical Philosophy
- 11–12 = Advanced refinement
- 10–12 = Improved results more structural reconfiguration
 Rib 10 can be treated with multiple techniques of which the most superior effect on waist/torso reshaping is not yet clear. The newer technique of rib shortening by segmental resection and plate fixation pulls its costal attachments more inward.
Rib 10 can be treated with multiple techniques of which the most superior effect on waist/torso reshaping is not yet clear. The newer technique of rib shortening by segmental resection and plate fixation pulls its costal attachments more inward.
Dr. Barry Eppley
World-Renowned Plastic Surgeon