

 In rib removal surgery for waist modification, the free-floating 11th and 12th ribs have historically been the primary targets. This preference is due to their relative accessibility and lack of distal structural attachments. However, more recent surgical experience and anatomical analysis have demonstrated that ribs 10 and 11 possess longer and wider segments than rib 12, making them more influential in achieving meaningful lower torso contouring. Among these, rib 10 has been shown to contribute most significantly to waist width and is therefore the most relevant rib for waist reduction. Anatomical studies indicate that removal of ribs 10 and 11 can reduce thoracoabdominal wall support by as much as 30%.
In rib removal surgery for waist modification, the free-floating 11th and 12th ribs have historically been the primary targets. This preference is due to their relative accessibility and lack of distal structural attachments. However, more recent surgical experience and anatomical analysis have demonstrated that ribs 10 and 11 possess longer and wider segments than rib 12, making them more influential in achieving meaningful lower torso contouring. Among these, rib 10 has been shown to contribute most significantly to waist width and is therefore the most relevant rib for waist reduction. Anatomical studies indicate that removal of ribs 10 and 11 can reduce thoracoabdominal wall support by as much as 30%.
 As a result, contemporary rib removal surgery now routinely includes rib 10. It is optimally approached through a vertical posterolateral incision, although in some cases it may be accessed via a lower oblique back incision. Removal of rib 10 requires a more extensive circumferential dissection to its subcostal cartilaginous end, which lacks a rigid attachment. In some patients, this cartilaginous end can be freely mobilized over the firmer attachment of rib 9 at the subcostal margin.
As a result, contemporary rib removal surgery now routinely includes rib 10. It is optimally approached through a vertical posterolateral incision, although in some cases it may be accessed via a lower oblique back incision. Removal of rib 10 requires a more extensive circumferential dissection to its subcostal cartilaginous end, which lacks a rigid attachment. In some patients, this cartilaginous end can be freely mobilized over the firmer attachment of rib 9 at the subcostal margin.
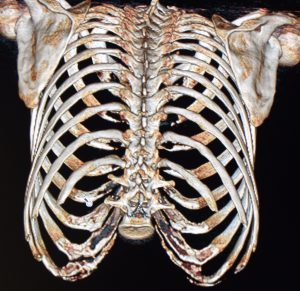
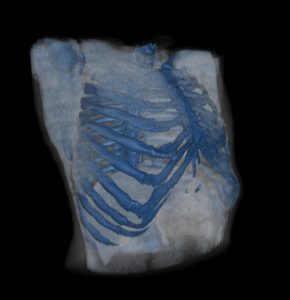
With rib 10 now considered standard treatment, the next logical and evolving question is whether rib 9 can also be addressed. Rib 9 is a typical rib, similar in morphology to ribs 3 through 8, with a long, curved, flattened shaft and an anterior attachment to the subcostal cartilages. It corresponds anatomically to the upper abdominal region and the inferior margin of the thoracic cage. Deep to rib 9 lie the liver on the right and the spleen on the left; more critically, the pleura of the lung lies immediately beneath it.
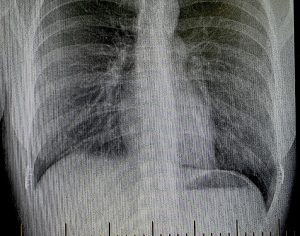
The relationship of rib 9 to the lung can be summarized as follows:
At rest (quiet breathing):
- Lung reaches rib 6 at the midclavicular line
- Rib 8 at the midaxillary line
- Rib 10 posteriorly
With deep inspiration:
- The lung may descend 1–2 rib levels, potentially reaching rib 9 laterally
Equally important is the position of the pleura, the outer lining of the lung. The parietal pleura extends lower than the lung itself:
- Rib 8 at the midclavicular line
- Rib 10 at the midaxillary line
- Rib 12 posteriorly
Thus, at rib 9—particularly along the midaxillary line—one is often below the lung but still within the pleural cavity.
Key anatomic takeaways:
- Rib 9 is generally below the lung at rest
- Rib 9 lies within the pleural reflection
- Deep inspiration can bring lung tissue down to rib 9
With an understanding of the rib–lung relationship, rib 9 can be surgically treated, but the method becomes the central question—removal versus fracture. A fracture technique is not feasible because the distal end of rib 9 is rigidly attached to the costal margin. Complete removal of four ribs (9, 10, 11, and 12) would be ill-advised, as it would leave a large unsupported area of the chest wall bilaterally.



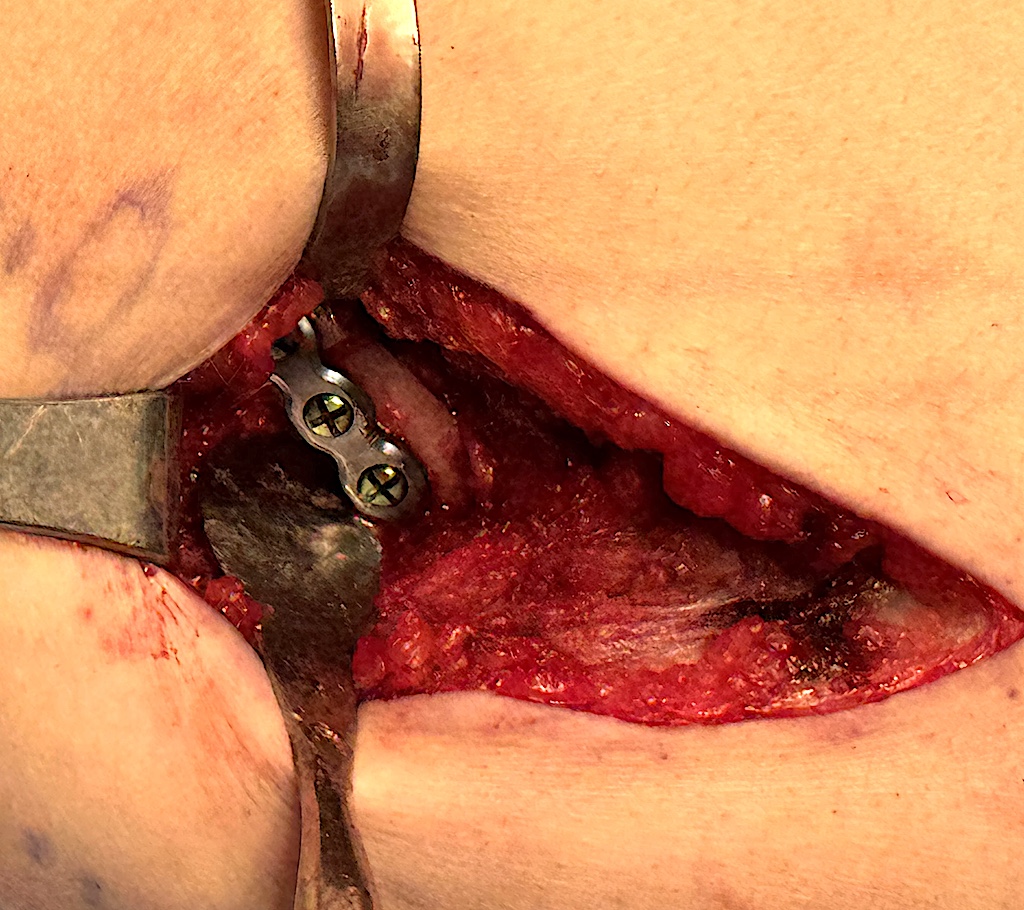
 An alternative and safer approach is a rib 9 osteotomy with segmental bone removal to shorten its arc, thereby achieving an outer width reduction effect. In this method, a mid-arc osteotomy is performed using a reciprocating saw. Once the two ends of the osteotomy are freed, the anterior segment of rib 9 is pushed posteriorly, allowing its cut end to overlap the more fixed posterior segment. This maneuver demonstrates how rib length can be reduced while still allowing approximation of the two ends. Typically, approximately 1.5 cm of rib length can be removed.
An alternative and safer approach is a rib 9 osteotomy with segmental bone removal to shorten its arc, thereby achieving an outer width reduction effect. In this method, a mid-arc osteotomy is performed using a reciprocating saw. Once the two ends of the osteotomy are freed, the anterior segment of rib 9 is pushed posteriorly, allowing its cut end to overlap the more fixed posterior segment. This maneuver demonstrates how rib length can be reduced while still allowing approximation of the two ends. Typically, approximately 1.5 cm of rib length can be removed.
The overlapping bone segment is excised, and the rib is stabilized using a four-hole rib fixation plate with two self-drilling 7-mm screws on each side.
 Segmental mid-arc removal of rib 9 represents a safe technique for ribcage narrowing. However, the magnitude of its contouring effect remains uncertain and is likely limited to the linear amount of bone removed (approximately 1.5 cm per side).
Segmental mid-arc removal of rib 9 represents a safe technique for ribcage narrowing. However, the magnitude of its contouring effect remains uncertain and is likely limited to the linear amount of bone removed (approximately 1.5 cm per side).
The next inevitable question is whether rib 8 could undergo a similar osteotomy-shortening technique. This is not a technical limitation, as it can be performed provided adequate surgical exposure is available. The more relevant—and currently unanswered—question is how much posterior displacement of the anterior rib segment would occur following such a procedure.
Dr. Barry Eppley
World-Renowned Plastic Surgeon