


Introduction
 Rib removal surgery — also known as rib resection or floating rib removal — is a body contouring procedure designed to create a smaller waistline and a more defined hourglass figure. As the procedure has evolved, its purpose has become focused on waist and torso narrowing, eliminating the final anatomical barrier to inward waist movement when traditional methods (diet, exercise, liposuction) prove insufficient. It can also address mid-torso narrowing by modifying ribs above the true floating ones.
Rib removal surgery — also known as rib resection or floating rib removal — is a body contouring procedure designed to create a smaller waistline and a more defined hourglass figure. As the procedure has evolved, its purpose has become focused on waist and torso narrowing, eliminating the final anatomical barrier to inward waist movement when traditional methods (diet, exercise, liposuction) prove insufficient. It can also address mid-torso narrowing by modifying ribs above the true floating ones.
Historically, the procedure targeted the floating ribs, 11 and 12, because they are not attached to the sternum. However, rib 10 is now frequently treated to enhance and elevate the waist-narrowing effect higher on the torso. Although rib 10 is traditionally described as a non-floating rib, my extensive clinical experience — including its use in rhinoplasty grafting and congenital ear reconstruction — demonstrates that it is not attached to the subcostal rib margin. In essence, rib 10 behaves as a floating rib, only positioned higher and with a more anterior orientation. Unlike ribs 11 and 12, rib 10 curves around the torso, which makes it more visually and structurally significant.
Because of this wrap-around configuration and its free cartilaginous end, rib 10 can produce a visible protrusion at the subcostal margin, especially in very thin patients. While this protrusion can be reduced through a small direct incision, it can also be corrected using the same posterior approach used for ribs 11 and 12. This dual benefit — aesthetic refinement and enhanced waist narrowing — further supports the inclusion of rib 10 in rib contouring surgery.
Case Study
This petite, thin female patient desired maximal waist narrowing through rib removal. She had previous breast and buttock implants and a history of hip implants, which were later removed due to infection. Owing to her thin frame, both the iliac crests and the ends of rib 10 were prominent, with greater prominence of rib 10 on the right side.

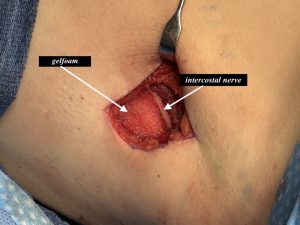 Under general anesthesia, with the patient in the prone position, ribs 10, 11, and 12 were marked. A small, vertical curvilinear incision was made between them. The outer third of ribs 11 and 12 were excised while carefully preserving the intercostal nerve on their undersides. An Exparel-soaked Gelfoam sponge was placed into each resected rib space for postoperative analgesia.
Under general anesthesia, with the patient in the prone position, ribs 10, 11, and 12 were marked. A small, vertical curvilinear incision was made between them. The outer third of ribs 11 and 12 were excised while carefully preserving the intercostal nerve on their undersides. An Exparel-soaked Gelfoam sponge was placed into each resected rib space for postoperative analgesia.

 Rib 10 was then dissected to its anterior cartilaginous end at the subcostal margin. All incisions were closed in multiple layers without the need for drains.
Rib 10 was then dissected to its anterior cartilaginous end at the subcostal margin. All incisions were closed in multiple layers without the need for drains.
Finally, bilateral iliac crest reductions were performed through the patient’s previous hip implant scars.



 At her three-day postoperative visit, she demonstrated noticeable waistline narrowing. Additionally, the previous rib 10 prominences were eliminated, and the iliac crest contours were reduced, creating a smoother and more tapered silhouette.
At her three-day postoperative visit, she demonstrated noticeable waistline narrowing. Additionally, the previous rib 10 prominences were eliminated, and the iliac crest contours were reduced, creating a smoother and more tapered silhouette.
Discussion
Traditionally, aesthetic rib modification has focused on the floating ribs 11 and 12, as they are nearest to the waistline and easiest to remove due to their unattached ends. However, addressing rib 10 enhances the overall contouring result because it extends low enough to influence the waistline’s shape. When approached through a properly placed incision, rib 10 can be accessed safely with reasonable visualization. This is particularly important since the pleura of the lung lies close at this level. By employing a tunnel rib delivery technique, the surgeon can reach and remove the cartilaginous end effectively and safely. Because it has a cartilaginous end far away from the incision, and there is a tendency for the cartilage to separate from its bony attachment, it is possible that the cartilage may fracture during rib removal. If it does it can no longer be grasped from the flank incision. It will either have to remain in placed or be removed by a small secondary incision over its end…depending upon how important removing the end is.
Key Points
-
Maximal waist narrowing is achieved when ribs 10, 11, and 12 are addressed through a single incision.
-
The prominent cartilaginous end of rib 10 can be removed without the need for a separate direct incision in most cases.
-
Rib removal effects are enhanced when combined with adjunct body contouring procedures, such as iliac crest reduction.
Barry Eppley, MD, DMD
World-Renowned Plastic Surgeon