

Barry Eppley, MD, DMD
World-Renowned Plastic Surgeon
Introduction
One of the most common shoulder muscle deformities is atrophy resulting from axillary nerve injury. The axillary nerve, a branch of the posterior cord of the brachial plexus (C5–C6), innervates the deltoid and teres minor muscles. Damage to this nerve—whether due to trauma, shoulder dislocation, or iatrogenic causes (e.g., surgical injury during shoulder procedures)—can lead to significant changes in shoulder contour.
When the axillary nerve is injured:
- Motor fibers to the deltoid are disrupted, resulting in loss of stimulation and subsequent muscle wasting and weakness.
- Over weeks to months, visible deltoid atrophy develops, producing a flattened shoulder contour. In cases involving loss of all three deltoid heads, the shoulder assumes a markedly bony or skeletonized appearance.
- Patients experience weakness in shoulder abduction (particularly between 15° and 90°) and difficulty with overhead movements due to loss of deltoid power.
When deltoid muscle atrophy becomes permanent, and nerve recovery is not possible, deltoid implants offer a purely aesthetic reconstructive solution. These implants restore shoulder contour but do not restore function or strength.
Deltoid implants are composed of solid silicone and have the following features:
- Made of soft, flexible solid silicone elastomer, available in varying degrees of firmness.
- Can be fashioned from standard contoured carving blocks or created via custom 3D design.
- Provide permanent and stable contour restoration.
Case Study
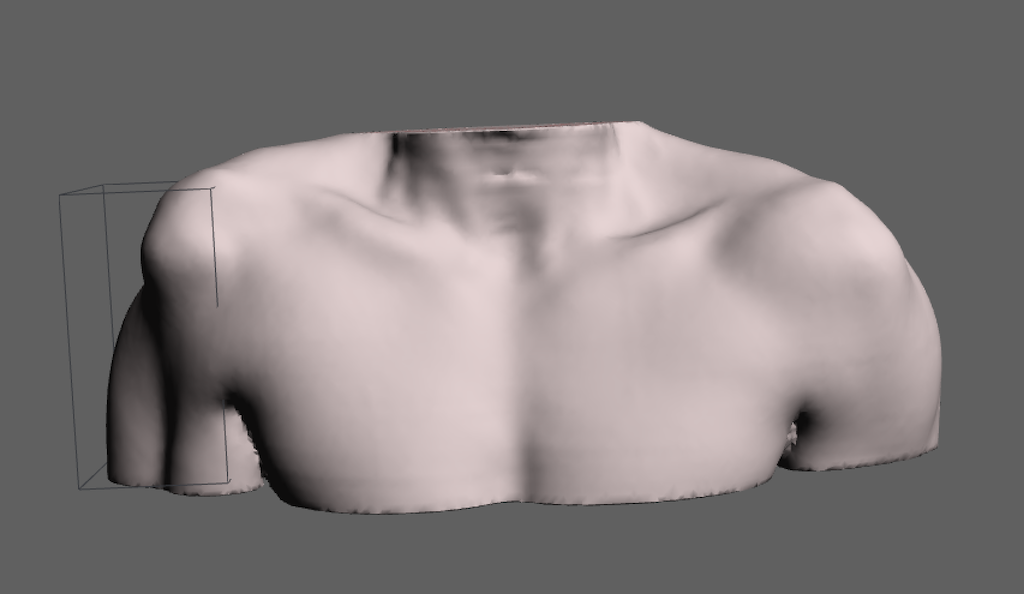
A young male patient sustained a right axillary nerve injury while making a tackle during a rugby match. No primary nerve reconstruction was attempted. Within six months, all three heads of the right deltoid had undergone profound atrophy, resulting in a bony shoulder contour with a prominently visible humeral head. The patient sought correction 12 years after the original injury.

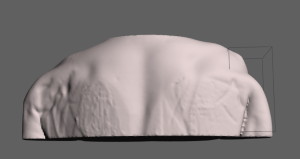

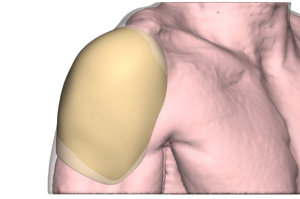 A 3D MRI of both shoulders was performed to evaluate the volume loss and guide implant design. Using the MRI data, a 3D reconstruction of the missing deltoid muscle was modeled as a single wraparound implant (although such an implant would not be surgically feasible due to placement and complication risks). From this model, implant volume and shape estimates were used to carve two separate solid silicone implants from preformed contoured blocks.
A 3D MRI of both shoulders was performed to evaluate the volume loss and guide implant design. Using the MRI data, a 3D reconstruction of the missing deltoid muscle was modeled as a single wraparound implant (although such an implant would not be surgically feasible due to placement and complication risks). From this model, implant volume and shape estimates were used to carve two separate solid silicone implants from preformed contoured blocks.

 Under general anesthesia, implant outlines and incision sites were marked on the shoulder. After making the incisions, the deltoid fascia was opened, and subfascial pockets were created in the atrophic space. The larger posterior implant was placed first, followed by the smaller anterior implant. It is critical to position the implants high on the shoulder to recreate a natural rounded contour.
Under general anesthesia, implant outlines and incision sites were marked on the shoulder. After making the incisions, the deltoid fascia was opened, and subfascial pockets were created in the atrophic space. The larger posterior implant was placed first, followed by the smaller anterior implant. It is critical to position the implants high on the shoulder to recreate a natural rounded contour.



 The incisions were closed in multiple layers, and a drain was placed in the posterior pocket.
The incisions were closed in multiple layers, and a drain was placed in the posterior pocket.
Early postoperative results demonstrated a marked improvement in shoulder contour, significantly reducing asymmetry between the two sides.
Postoperative Care
- Limit right arm range of motion for several weeks to reduce the risk of seroma formation.
- Gradual return to normal activity after 3–4 weeks.
- Drain removal in 7–10 days.
- Avoid heavy lifting or strenuous workouts for 6–8 weeks.
Discussion
The only effective method for restoring shoulder contour after deltoid muscle loss due to nerve injury is implant-based reconstruction. While functional recovery is not achievable, the restoration of a rounded shoulder contour provides significant aesthetic and psychological benefits, improving symmetry and body balance.
Solid silicone implants offer long-term stability, and implant migration is exceedingly rare. Implants may be either standardized contoured blocks tailored to the patient’s anatomy or custom-designed from 3D MRI data.
Despite their effectiveness, deltoid implants are not complication-free. Because they are placed in tissue lacking normal muscle thickness, seroma formation is a recognized issue. The use of drains reduces this risk, though occasional needle aspirations may be necessary in the first postoperative month.
From an aesthetic standpoint, lower-edge implant visibility or edging can occur depending on implant design and silicone firmness. While perfect symmetry is rarely attainable, most patients find the initial improvement satisfactory. In select cases, secondary implant refinement can further enhance symmetry and contour.
Key Points
- Deltoid muscle denervation leads to severe muscle wasting and shoulder asymmetry.
- Silicone implants offer reliable restoration using a two-piece placement technique that minimizes risk.
- High incisional placement helps achieve a natural, rounded shoulder contour.
Barry Eppley, MD, DMD
World-Renowned Plastic Surgeon