

Scars from most plastic surgery procedures are an inevitable outcome. Most plastic surgery operations require an incision, and when this is necessary as it almost always is, a scar will result. While many incisions (and subsequent scars) can be relatively ‘hidden’ dependent upon the procedure (e.g., facelift, blepharoplasty), many plastic surgery procedures on the body can not. (e.g., breast reduction, arm lift) As a result, many procedures require the acceptance of a scar for the procedure’s other benefits. Or to put it another way….make sure the scars are a more acceptable ‘solution’ than the originial problem.
For some procedures, the acceptance of a scar is relatively easy as it lays in a relatively non-visible location. Procedures such as facelifts, tummy tucks, or thigh lifts place scars in favorable locations that are very tolerable and patients do not usually have a problem with their presence. In other operations such as breast lifts and arm lifts, the scars are anything but hidden and the decision for that procedure can be a more delicate quandry. In the spirit of trading off one problem for another, I advise patients to be sure that the creation of a scar will be viewed as less of a problem than their original concern. In the end, cosmetic plastic surgery is about making the patient feel better about themselves and their areas for which they are self-conscious. It does the patient no good, for example, if the arm from an armlift is much smaller around but the patient hates the scar. In this example, the patient is still is not comfortable with their arm and nothing has been achieved but a surgical exercise.
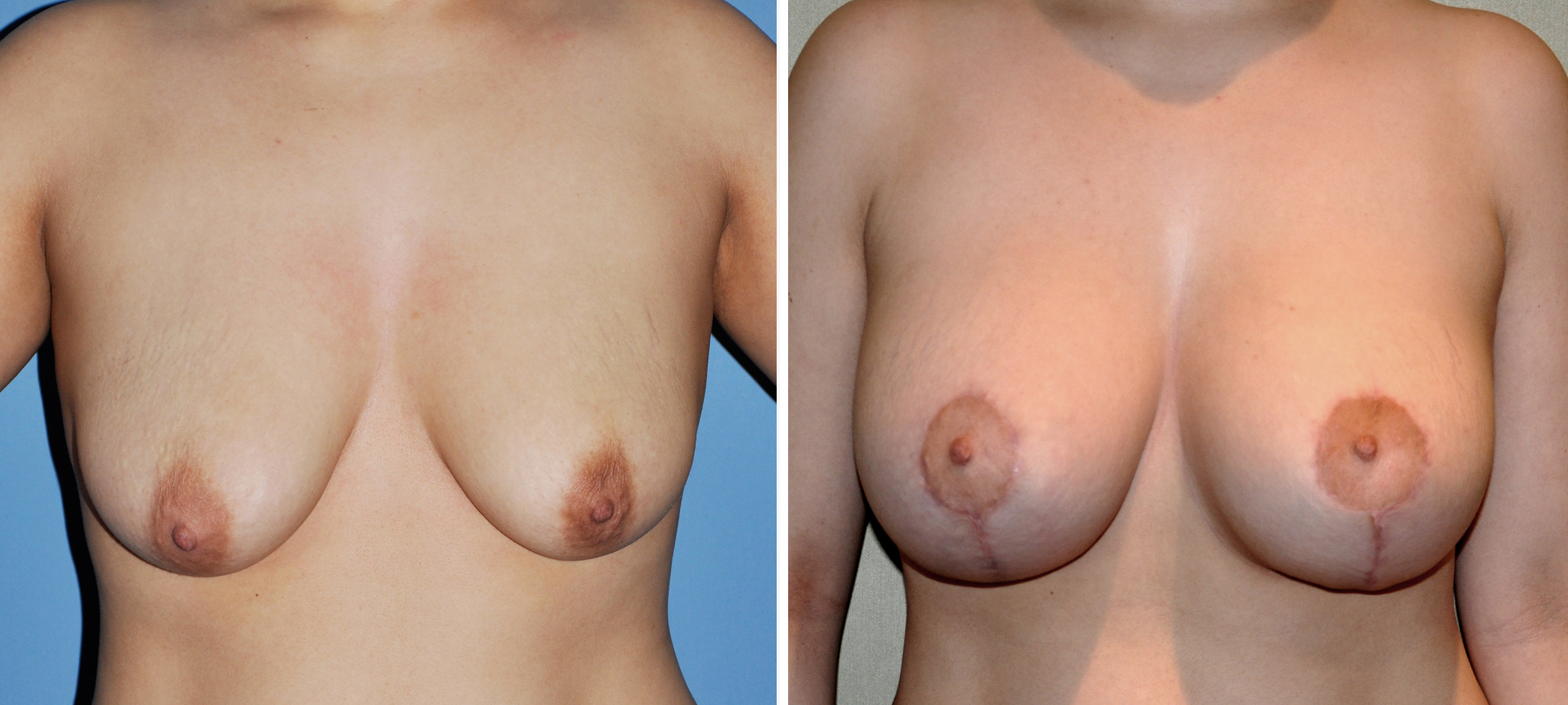 There are certain plastic surgery procedures to which scarring is of an utmost concern. I find that the breast lift or mastopexy is the #1 plastic surgery procedure to which this scar concern applies. Which is better…a breast that sags with no scar or a better shaped breast with visible scars? That can be a tough call for some patients and obviously depends upon how severe the initial problem is. While a patient must make the final call about a scar vs. improvement trade-off, I have found a simple way to make this decision. If when talking about the scar, the patient quickly says and indicates that…..what do I care about that scar, who would want to live with this? (or some variation thereof) Then this is a safe scar bet. Conversely, if the patient slowly starts shaking their head, looks concerned, or says they are not sure or have to think about it, then I will not do the procedure. A scar is not something you should have to think very much about. If you have to talk yourself into thinking the scar will be fine, it will likely not be. Furthermore, once a scar is on the patient, I have no magic eraser to get it off. There will always be another day or sometime later in life in which the concept of a scar may be more appealing.
There are certain plastic surgery procedures to which scarring is of an utmost concern. I find that the breast lift or mastopexy is the #1 plastic surgery procedure to which this scar concern applies. Which is better…a breast that sags with no scar or a better shaped breast with visible scars? That can be a tough call for some patients and obviously depends upon how severe the initial problem is. While a patient must make the final call about a scar vs. improvement trade-off, I have found a simple way to make this decision. If when talking about the scar, the patient quickly says and indicates that…..what do I care about that scar, who would want to live with this? (or some variation thereof) Then this is a safe scar bet. Conversely, if the patient slowly starts shaking their head, looks concerned, or says they are not sure or have to think about it, then I will not do the procedure. A scar is not something you should have to think very much about. If you have to talk yourself into thinking the scar will be fine, it will likely not be. Furthermore, once a scar is on the patient, I have no magic eraser to get it off. There will always be another day or sometime later in life in which the concept of a scar may be more appealing.
The other issue about a scar is that not all scars, no matter how visible or well placed, will always turn out well. Even in routinue procedures, a patient’s scar can turn out poorly no matter how well the operation is performed. Scar hypertrophy and the possible new for scar revision later is always a possibility. Patients have to be informed of this possibility and have to be willing to accept this poor outcome. While scar revision is always possible, there is no guarantee that scar revision will always be successful.
Dr. Barry Eppley
Indianapolis, Indiana