

Custom jawline implants can be very effective for facial asymmetry when the problem is mainly a contour or volume deficiency of the mandibular border, angle, or chin, especially if one side is underprojected. With modern patient-specific / custom implants, CT/CBCT-based virtual planning an be done to design different right and left dimensions, which improves fit and lets the implant target exact asymmetries more accurately than stock implants ever could.
They are not the best solution when the asymmetry is primarily from occlusion, skeletal cant, jaw position, condylar issues, or bite-related mandibular deviation. In those cases, orthodontics and/or orthognathic surgery should be done first for overall skeletal realignment, with implants used only as an adjunct for residual contour imbalance which is almost always necessary. 3D imaging is important because facial asymmetry is a true 3D problem and standard 2D assessment can miss the source of the deformity.
In practice, custom jawline implants are best for:
- Unilateral mandibular angle/body deficiency
- Hemimandibular contour deficiency
- Residual asymmetry after prior orthognathic surgery
- Patients with a stable bite who want skeletal border equalization rather than jaw repositioning
Main advantages:
- side-to-side customization
- stronger control of jawline width, angle, and inferior border shape
- better adaptation to native anatomy
- potentially shorter, more precise surgery through CAD/CAM planning.
Main limitations and risks:
- implants improve shape, but do not perfectly correct soft-tissue asymmetry
- if the diagnosis is wrong, the implant can “camouflage” rather than solve the true problem
- risks include infection, malposition/asymmetry and need for revision.
An adequate workup includes:
- front, side, oblique and basal view picture analysis
- bite/occlusion assessment
- CBCT or CT with 3D planning
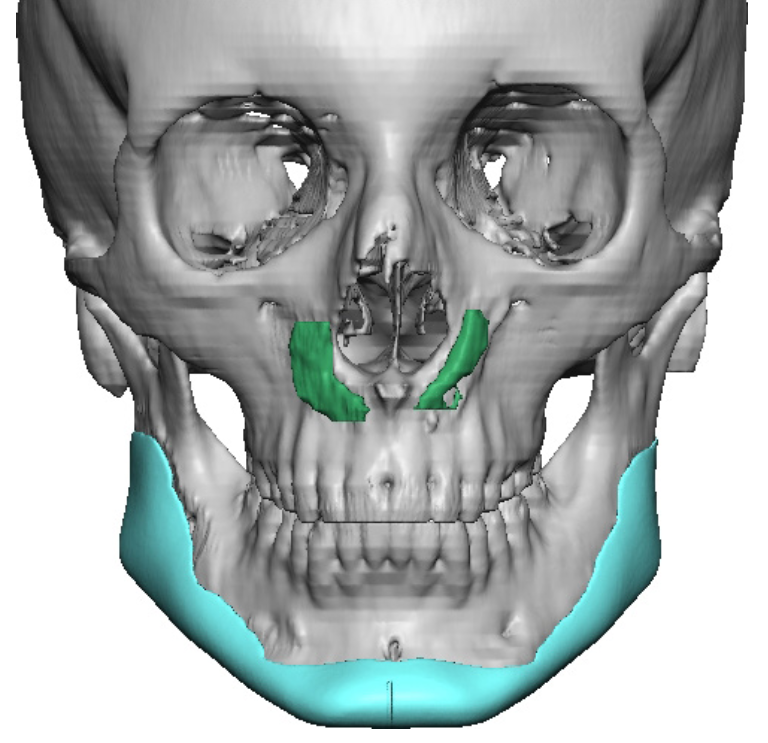
Case Example
![]()
 This female had right facial asymmetry which had been previously treated by a standard implant approach over a decade ago. This included a right Goretex block and sheet augmentation of the right jawline, a sliding genioplasty and left Goretex jaw implants. The right implants were placed and removed twice due to infection. No implants remained on the left side as a result. This left her with a more pronounced facial asymmetry than that of her original bony jaw asymmetry.
This female had right facial asymmetry which had been previously treated by a standard implant approach over a decade ago. This included a right Goretex block and sheet augmentation of the right jawline, a sliding genioplasty and left Goretex jaw implants. The right implants were placed and removed twice due to infection. No implants remained on the left side as a result. This left her with a more pronounced facial asymmetry than that of her original bony jaw asymmetry.
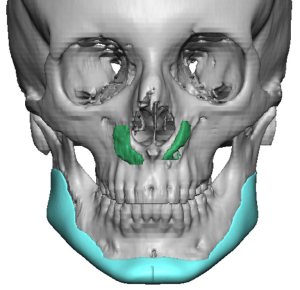
 A custom jawline implant was designed for improved jaw asymmetry based on removal of the right sided Goretex implant material.
A custom jawline implant was designed for improved jaw asymmetry based on removal of the right sided Goretex implant material.
Due to her history of implant infections she did not want to use an intraoral approach. She opted for a total three external incisional approach.

 Initially a right transcutaneous jaw angle incision was made and the Goretex implant material identified by its white appearance. The entire implant and screws were removed from the jaw angle and body area.,
Initially a right transcutaneous jaw angle incision was made and the Goretex implant material identified by its white appearance. The entire implant and screws were removed from the jaw angle and body area.,
 The submental and left jaw angle incisions were made and the subperiosteal pockets and tunnel connections were made along the entire jawline. The implant was inserted through the submental incision and the chin section aligned and secured with two screws.
The submental and left jaw angle incisions were made and the subperiosteal pockets and tunnel connections were made along the entire jawline. The implant was inserted through the submental incision and the chin section aligned and secured with two screws.

 Secure central chin positioning then allows the jaw angle portions of the implant to be positioned and secured.
Secure central chin positioning then allows the jaw angle portions of the implant to be positioned and secured.

 The incisions were closed with multi-layer resorbable sutures.
The incisions were closed with multi-layer resorbable sutures.

 The improvement in the jaw asymmetry could be immediately appreciated.
The improvement in the jaw asymmetry could be immediately appreciated.
Discussion
Here’s a practical treatment-planning framework followed by a side-by-side comparison of custom jawline implants, double jaw (Bimax) surgery, and fat grafting—for facial asymmetry cases.
1. Treatment-Planning Framework for Facial Asymmetry
Step 1: Identify the type of asymmetry (this is everything)
A. Skeletal positional (jaw is “shifted”)
- Chin deviation
- Occlusal cant (tilted bite)
- Midline mismatch
- Condylar asymmetry
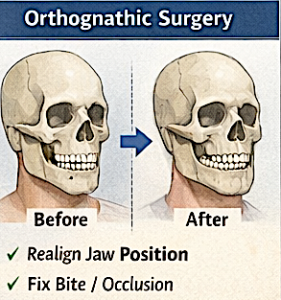
Primary solution: Double Jaw surgery
B. Skeletal deficiency (one side underdeveloped)
- Smaller mandibular angle/body on one side
- Flat gonial angle
- Chin asymmetry without bite issues
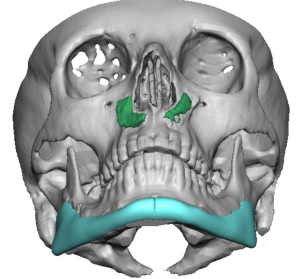
Primary solution: Custom jawline implant
C. Soft tissue asymmetry
- Volume differences (fat/muscle)
- Skin thickness differences
- Post-traumatic or idiopathic soft tissue imbalance
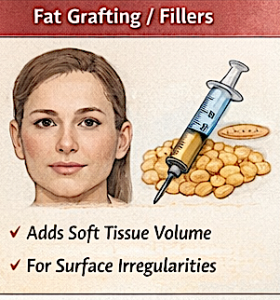
Primary solution: Fat grafting ± fillers
D. Mixed (very common)
- Mild skeletal shift + contour deficiency + soft tissue imbalance
?? Combination approach
2. Decision Algorithm (Simplified)
- Is the bite off?
- YES ? Double Jaw surgery (foundation problem)
- NO ? Go to next
- Is the bone shape asymmetric?
- YES ? Custom implant
- NO ? Go to next
- Is it just soft tissue?
- YES ? Fat grafting
- Is it subtle/mixed?
- Combine (very common in real cases)
3. Modality Comparison (Real-World Use)
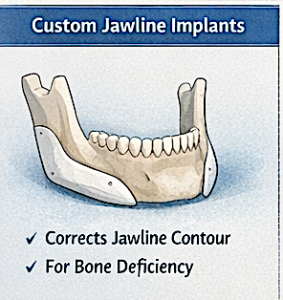
Custom Jawline Implants
Best for:
- Unilateral mandibular hypoplasia
- Jawline contour asymmetry
- Normal occlusion
Strengths
- Precise side-to-side correction
- Permanent structural change
- Can widen, lengthen, and reshape jaw
Limitations
- Does NOT fix jaw position or bite
- Soft tissue asymmetry may persist
- Requires accurate diagnosis (easy to over/under-correct)
Think of it as:
“Adding missing bone where it should have been”
Double Jaw Surgery
Best for:
- Chin deviation from skeletal shift
- Occlusal cant
- Bite problems (malocclusion)
- Mandibular or maxillary asymmetry in position
Strengths
- Corrects root cause
- Improves function + aesthetics
- Re-centers entire lower face
Limitations
- Major surgery
- Longer recovery
- May still need contour refinement afterward
Think of it as:
“Repositioning the entire jaw framework”
Fat Grafting (± Fillers)
Best for:
- Soft tissue volume asymmetry
- Mild contour irregularities
- Adjunct to skeletal correction
Strengths
- Minimally invasive
- Natural tissue
- Good for fine-tuning
Limitations
- Unpredictable resorption
- Not structural
- Often requires repeat sessions
Think of it as:
“Camouflaging or blending surface asymmetry”
4. Pattern-Based Treatment Guide (Most Useful Section)
Pattern 1: Chin deviates to one side + bite off
Cause: Skeletal shift
Treatment:
- Double Jaw surgery
- ± custom implant for refinement
Pattern 2: One jaw angle smaller/less defined (bite normal)
Cause: Mandibular deficiency
Treatment:
- Custom jawline implant (unilateral or asymmetric design)
Pattern 3: Jaw looks asymmetric but bone is symmetric (illusion)
Cause: Soft tissue or muscle imbalance
Treatment:
- Fat grafting / fillers
- ± Botox (masseter asymmetry)
Pattern 4: Post-Double Jaw surgery residual asymmetry
Cause: Residual contour difference
Treatment:
- Custom implant (very common use case)
- ± fat grafting
Pattern 5: Mild asymmetry (common in most people)
Cause: Mixed small differences
Treatment:
- Often non-surgical or minimal
- Filler / fat grafting
- Sometimes small custom implant
Pattern 6: Hemimandibular hypoplasia (one side underdeveloped)
Treatment:
- Custom jawline implant (core)
- ± fat grafting for soft tissue match
- Rarely orthognathic unless occlusion involved
5. Common Planning Mistakes (Critical)
- Using implants when the jaw is actually shifted
- Ignoring occlusion
- Expecting implants to fix soft tissue asymmetry
- Overcorrecting one side ? new asymmetry
- Not using 3D planning (huge mistake in any asymmetry case)
Key Case Insights
- Facial asymmetry is almost always multi-dimensional—single-solution thinking leads to suboptimal results.
- 2D planning (eyeballing it) rarely works well for a 3D bony asymmetry problem.
- infections after jaw angle implants placed through an intraoral approach is avoided secondarily by transcutaneous incisional access.
Dr. Barry Eppley
Plastic Surgeon