

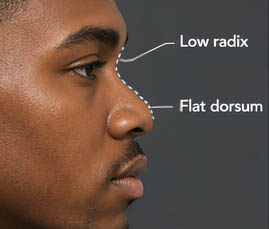
Nasal dorsal augmentation involves increasing the height and/or improving the contour of the nasal bridge (dorsum). It is a common component of rhinoplasty, particularly in patients with a low or flat nasal bridge or an irregular dorsal contour.
Common Indications
- Low nasal bridge (common in many Asian, African, or revision rhinoplasty patients)
- Saddle nose deformity (due to trauma, prior surgery, or congenital causes)
- Dorsal irregularities or asymmetry
- Desire for a more defined nasal profile
Methods of Augmentation
1. Autologous Grafts (Patient’s Own Tissue)
- Septal cartilage – first-line option when available
- Auricular (ear) cartilage – naturally curved; useful for moderate augmentation
- Costal (rib) cartilage – preferred for significant augmentation or revision cases
Advantages: Biocompatible, low risk of infection or extrusion
Disadvantages: Donor site morbidity; potential warping (especially rib cartilage)
2. Alloplastic Implants (Synthetic Materials)
- Silicone
- ePTFE (Gore-Tex)
- Medpor (porous polyethylene)
Advantages: No donor site; predictable shape
Disadvantages: Higher risk of infection, extrusion, and long-term complications
3. Diced Cartilage Techniques
- Diced cartilage wrapped in fascia (e.g., temporalis fascia)
- Useful for achieving smooth contour and avoiding sharp edges or visibility
Surgical Considerations
- Skin thickness (thin skin increases visibility risk; thick skin limits definition)
- Desired dorsal height and radix position
- Structural support and integration with tip projection
- Avoidance of over-augmentation for a natural appearance
Potential Complications
- Infection
- Implant extrusion (more common with synthetic materials)
- Warping or resorption (cartilage grafts)
- Irregular contour or asymmetry
Key Principle
The goal is not simply to increase dorsal height, but to create a natural dorsal aesthetic line that harmonizes with the nasal tip, radix, and overall facial proportions.
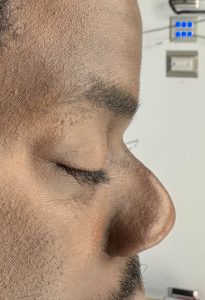
Case Example
This male patient had a prior rhinoplasty using a rib graft to reconstruct a low radix/dorsum and augment the tip. While he was satisfied with the tip, the dorsal rib graft had warped, resulting in deviation and insufficient length to adequately augment the entire dorsum. This created a prominent dorsal hump on profile view.
Due to concerns about postoperative pain, the patient declined another rib graft harvest and opted for an implant.

 Through an open rhinoplasty approach:
Through an open rhinoplasty approach:
- The warped dorsal rib graft was removed
- The tip reconstruction was preserved
- Dissection was extended to the frontonasal junction
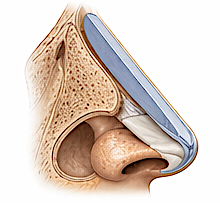
- An 8 mm thick block of ePTFE was hand-carved into a 4 cm implant with a tapered thickness toward the supratip
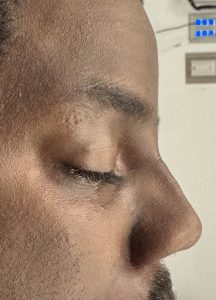 The implant was inserted, secured to the tip cartilages, and the rhinoplasty was closed. The dorsal contour improvement was immediate and aesthetically favorable.
The implant was inserted, secured to the tip cartilages, and the rhinoplasty was closed. The dorsal contour improvement was immediate and aesthetically favorable.
Discussion
In African American patients, dorsal augmentation often plays a more significant aesthetic role. The goal is not simply to raise the bridge, but to create a balanced, natural-appearing dorsum that respects the patient’s ethnic identity.
Key Anatomical Features
Common (though not universal) characteristics include:
- Low or flat nasal dorsum
- Thick, sebaceous skin envelope
- Weaker cartilaginous framework
- Wider nasal base with softer tip support
These features directly influence both technique selection and expected outcomes.
Surgical Goals
- Create a defined but not over-projected dorsal line
- Maintain ethnic harmony (avoid over-narrowing or over-“Westernization”)
- Improve tip support and projection along with dorsal augmentation
- Establish a smooth radix-to-tip aesthetic line
Preferred Techniques
1. Rib Cartilage
- Most commonly used for significant dorsal augmentation, particularly dorso-columellar augmentation
- Provides sufficient volume and structural support for both dorsum and tip
- Solid rib grafts may warp, so diced rib graft techniques are often preferred
Adequate graft length is critical. Insufficient rib harvest can lead to incomplete augmentation. Surgeon experience plays a major role in graft quality and quantity.
2. Alloplastic Implants
- Includes silicone, Gore-Tex, and Medpor
Considerations:
- Higher infection risk
- Generally less favored in primary cases
- Often used as a salvage option after failed rib graft augmentation
Important Technical Considerations
Radix Positioning
- Often low in African American patients
- Requires augmentation extending from the radix down to the tip for balanced profile improvement
Skin Thickness
- Thick skin helps conceal graft or implant edges
- Allows for greater augmentation without visible irregularities
Combined Implant–Rib Graft Techniques
While implants are generally avoided in primary large dorsal augmentations, they can be effective in revision or salvage cases when rib graft results are inadequate.
Key points:
- Implants should not be used for tip support or extension
- They are best limited to the dorsal region above the supratip
- Combined approaches may occur unintentionally due to inadequate initial planning
This case represents a two-stage augmentation: an initial rib graft followed by implant placement due to graft insufficiency. Ideally, preoperative planning should address contingencies if rib graft volume proves inadequate, particularly in cases requiring substantial dorsal dorso-columellar augmentation (dorsum and tip).
Dr. Barry Eppley
Plastic Surgeon