

Many men seek the high cheekbone look as a method to enhance their facial appearance. I view such augmentation very similarly to the jawline in that it is really a long horizontal facial augmentation effect….with the exception of not crossing the nose area in the midline. (unlike a jawline implant which crosses the chin area and is a very important part of the three corner augmentation effect) The high cheekbone look is called that because it augments the highest part of the cheek and out onto the thin but highly positioned zygomatic arch. This is to be differentiated from standard cheek implants which creates a lower fuller augmentation in the major cheekbone area which is usually only desired by women or either gender affected by significant facial lipoatrophy. (where the face already has a skeletonized appearance)
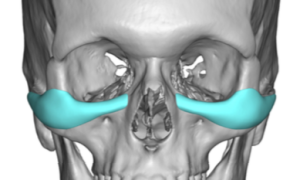 In designing custom infraorbital-malar implants, which is the most effective approach to getting the high cheekbone look, the most common design ‘error’ is making them too big. It is amazing how just a millimeter or two one way or the other in the midface area makes a big difference. This is due to the thin soft tissue cover where the implant is more easily seen. This is unlike custom jawline implants where the reality is that one millimeter to two either way rarely makes any visible external distance. And like all facial implants, no matter how much thought and belief one has in the implant design beforehand, the patient never really knows how they will feel about it until the actually wear it. (have it surgically implanted)
In designing custom infraorbital-malar implants, which is the most effective approach to getting the high cheekbone look, the most common design ‘error’ is making them too big. It is amazing how just a millimeter or two one way or the other in the midface area makes a big difference. This is due to the thin soft tissue cover where the implant is more easily seen. This is unlike custom jawline implants where the reality is that one millimeter to two either way rarely makes any visible external distance. And like all facial implants, no matter how much thought and belief one has in the implant design beforehand, the patient never really knows how they will feel about it until the actually wear it. (have it surgically implanted)
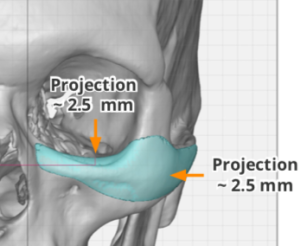 Where was has to be careful in custom infraorbital-malar implants is where the implant turns the corner from infraorbital to malar. This is commonly the thickest part of the implant where the anterior and posterior extensions of the implant usually fade in thickness from it. It would be very rare that anyone ever needs more than 3.5 or 4mms thickness. Most patients don’t need more than 3mms and some as little s 2.5mms in thickness.
Where was has to be careful in custom infraorbital-malar implants is where the implant turns the corner from infraorbital to malar. This is commonly the thickest part of the implant where the anterior and posterior extensions of the implant usually fade in thickness from it. It would be very rare that anyone ever needs more than 3.5 or 4mms thickness. Most patients don’t need more than 3mms and some as little s 2.5mms in thickness.
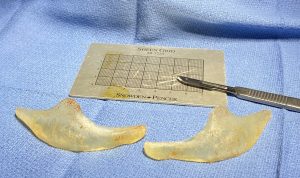
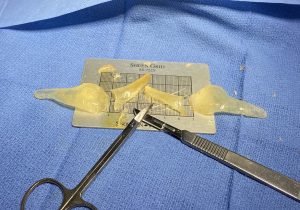

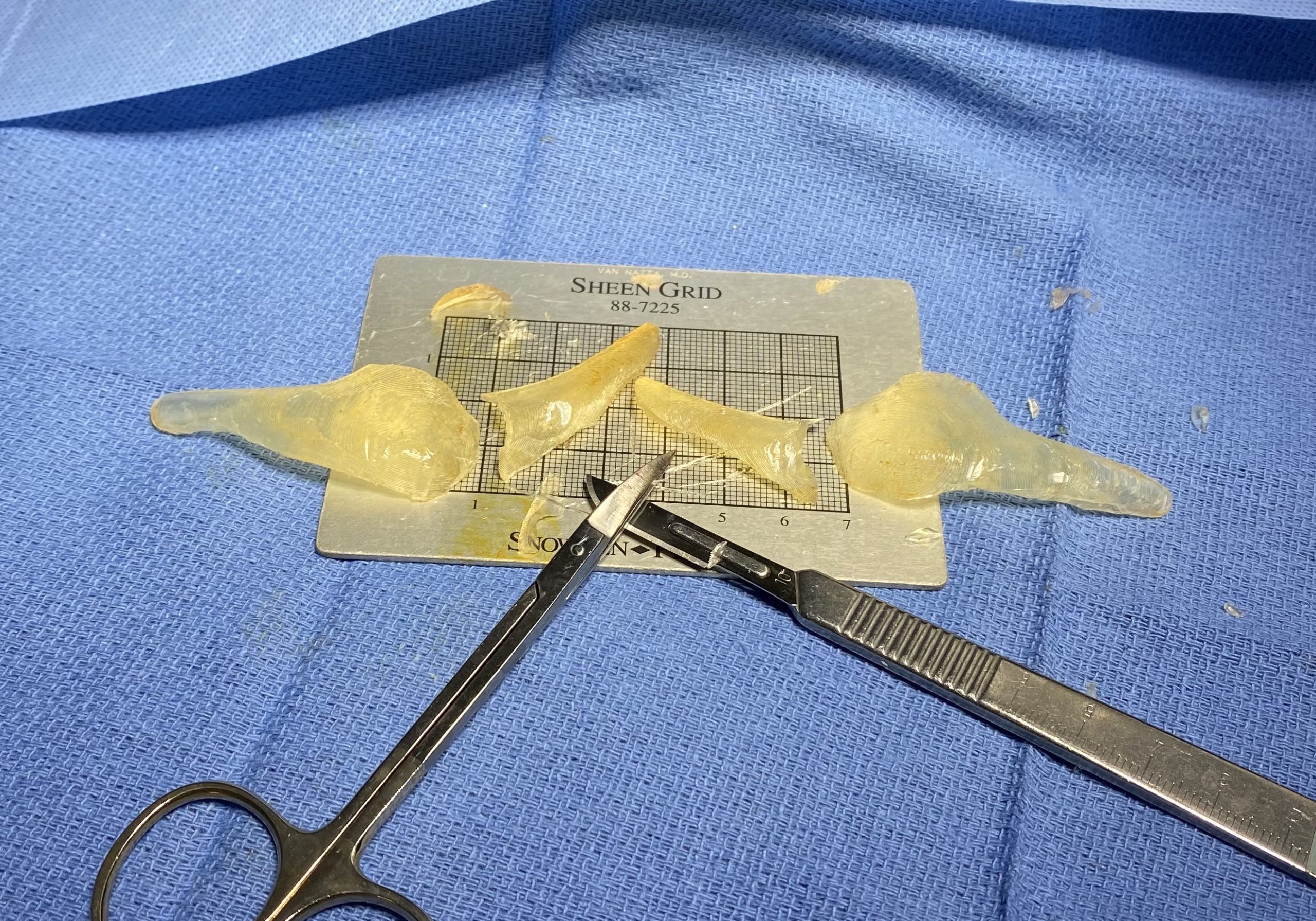
 But when a patient determines that their custom infraorbital-malar implants are too much, the good news is that there is an effective solution that does not require making a new implant. Intraoperative reduction of the implant can be done by explantation, sculpting the implant down to the desired shape and thickness and immediate reimplantation.,
But when a patient determines that their custom infraorbital-malar implants are too much, the good news is that there is an effective solution that does not require making a new implant. Intraoperative reduction of the implant can be done by explantation, sculpting the implant down to the desired shape and thickness and immediate reimplantation.,
The only question on secondary infraorbital-malar implant adjustments are whether it can/should be done through the original eyelid incision or done from below intraorally. It can be done either way and that is really up to the patient. Some patients do not want to go through their eyelids again and incur any risk of lower eyelid deformities. (although secondarily this is very unlikely with an established pocket) Then the intraoral approach can be used. While this is rarely an approach for placement of custom infraorbital-malar implants due to the more difficult access for proper pocket dissection, when an established pocket exists there is no risk of implant displacement out of the established pocket.
Dr. Barry Eppley
Indianapolis, Indiana