

In aesthetic testicular enhancement surgery a wide variety of scrotal interventions and abnormalities can be encountered. The most common are atrophic testicular changes with below normal sizes…which is of course why they are presenting for the surgery. But numerous other entities may be found from penile pump extensions to various injectable. While every non-autologous entity in the scrotum poses potential concerns when a large testicle implant is going to be placed, none are more potentially problematic than permanent fillers like silicone.
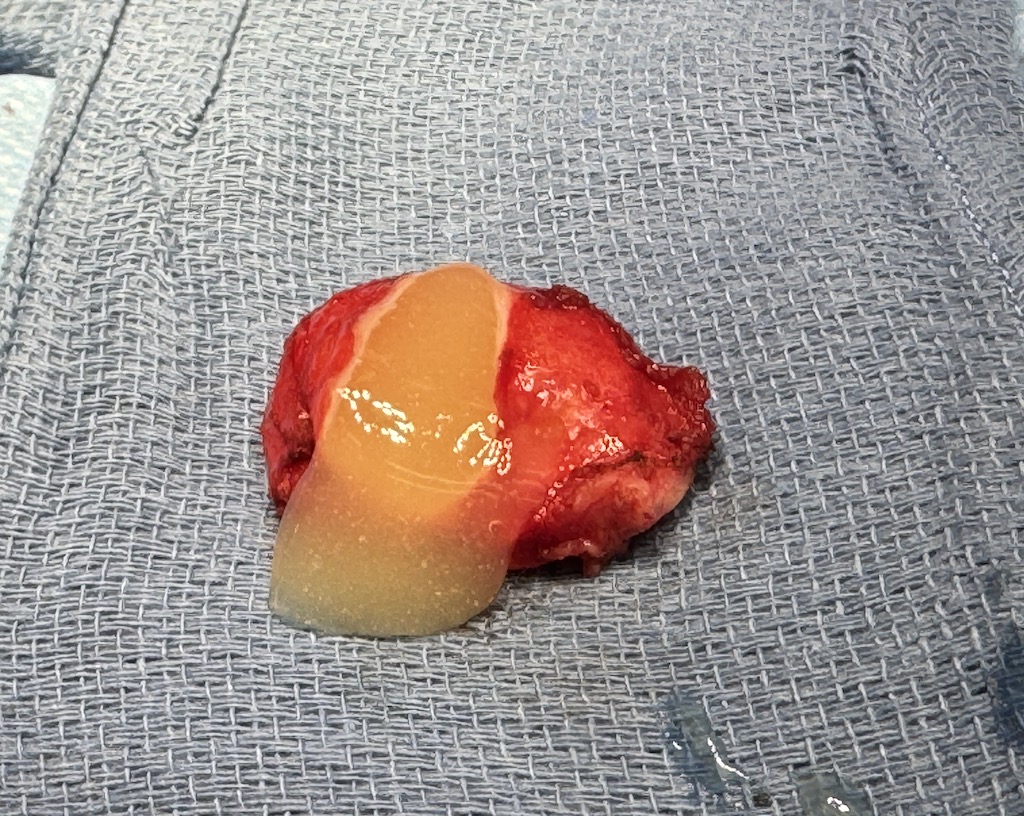
 Silicone injections have been used for a long time with well known potential adverse soft tissue reactions. They are most successful when placed in the face using a micro droplet technique…which means a little bit of silicone oil interspersed amidst a much larger surface area of healthy soft tissue. Biologically the oil is tolerated because it is does not tip the balance between tolerance and an inflammatory reaction due to low foreign body load. But when used for augmentations in the body it is easy to place larger loads of materials that end up as encased balls of oil. Despite the isolated volume of foreign material in these encapsulated masses many patients develop no inflammatory response to them. (although some do)
Silicone injections have been used for a long time with well known potential adverse soft tissue reactions. They are most successful when placed in the face using a micro droplet technique…which means a little bit of silicone oil interspersed amidst a much larger surface area of healthy soft tissue. Biologically the oil is tolerated because it is does not tip the balance between tolerance and an inflammatory reaction due to low foreign body load. But when used for augmentations in the body it is easy to place larger loads of materials that end up as encased balls of oil. Despite the isolated volume of foreign material in these encapsulated masses many patients develop no inflammatory response to them. (although some do)

 In considering a patient for testicular enhancement implants if there is a history of silicone injections into the scrotum the removal of the silicone masses should be done first and the implants later. In my limited experience of two cases were large silicone masses were removed, one with the testicles removed as well, they both developed complications. One was an infection that occurred weeks after surgery resulting in implant removals for resolution.
In considering a patient for testicular enhancement implants if there is a history of silicone injections into the scrotum the removal of the silicone masses should be done first and the implants later. In my limited experience of two cases were large silicone masses were removed, one with the testicles removed as well, they both developed complications. One was an infection that occurred weeks after surgery resulting in implant removals for resolution.

 The silicone removal case that resulted in the planned testicle implant removals for complete material removal, a chronic fluid collection (seroma) developed. Despite the use of drains, the seroma required one year of aspirations but finally resolved and the implants were able to be maintained.
The silicone removal case that resulted in the planned testicle implant removals for complete material removal, a chronic fluid collection (seroma) developed. Despite the use of drains, the seroma required one year of aspirations but finally resolved and the implants were able to be maintained.
Despite the encapsulation of silicone oil in the scrotum and its removal I believe it increases the risk of postoperative complications when implants are placed concurrently with the removal. As a result the use of testicle implants should be placed secondarily into the scrotum or perhaps avoided completely.
When it comes to other types of non-permanent injectables that are placed into the scrotum (e.g., fat, saline or hyaluronic acid fillers) I see no problem with implants placed into scrotums that have been injected into them.
Dr. Barry Eppley
World-Renowned Plastic Surgeon