

Asymmetry of the chin is not uncommon and has various causes. Fundamentally it can be either due to how jaw has developed along its two sides with the chin at its end reflecting the difference between the two sides or can be directly due to asymmetry of the chin bone itself. That diagnosis is very relevant and can affect how chin asymmetry is best treated.
Direct treatment of chin asymmetry consists of modifying the chin bone itself. One option is to contour the external shape of the chin bone through shaving or burring of the more prominent side or augmentation of the deficient side based on which method addresses the asymmetry the best. This can be done either intraoral or externally through a submental incision with each incisional approach having their unique advantages and disadvantages.
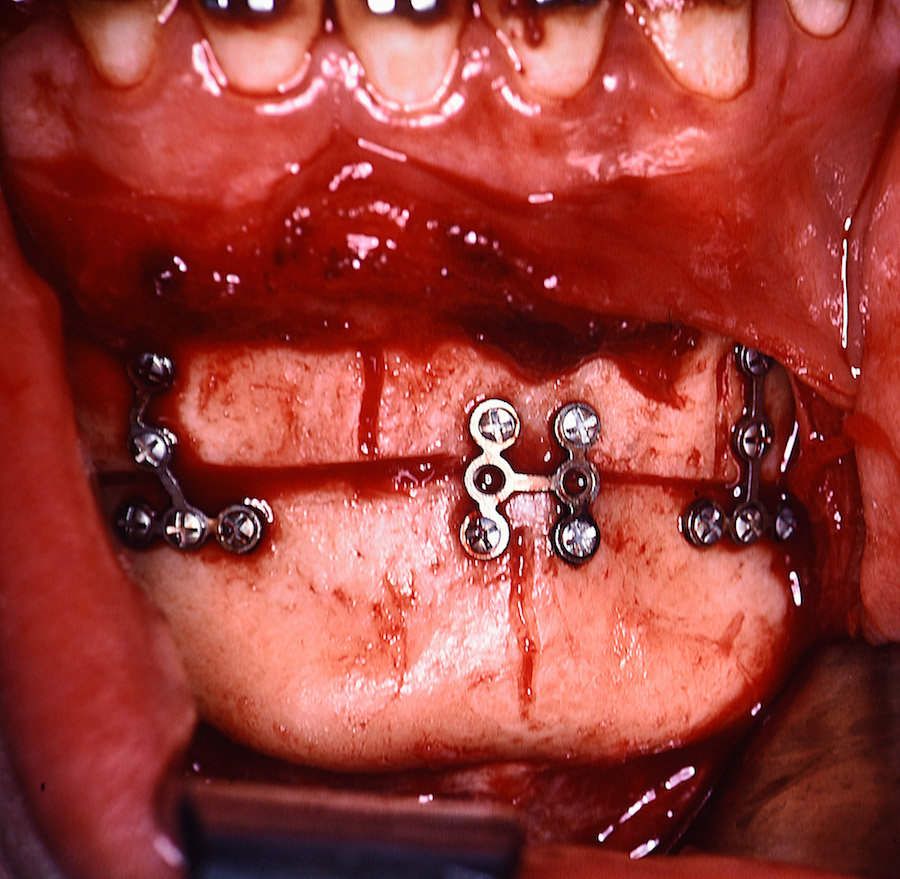 The second option of direct chin asymmetry treatment is an intraoral osteotomy technique. Like a traditional sliding genioplasty a horizontal bone cut is made. But rather than moving the bone forward it is shifted to the side. (lateral sliding genioplasty) The larger asymmetric side is shifted to the opposite side. How far it shifts is guided by the midline of the chin point to the dental midline between the lower central incisors. This amount of movement is also determined preoperatively by x-ray measurements. Once the optimal midline position is obtained it is secured there with small plates and screws.
The second option of direct chin asymmetry treatment is an intraoral osteotomy technique. Like a traditional sliding genioplasty a horizontal bone cut is made. But rather than moving the bone forward it is shifted to the side. (lateral sliding genioplasty) The larger asymmetric side is shifted to the opposite side. How far it shifts is guided by the midline of the chin point to the dental midline between the lower central incisors. This amount of movement is also determined preoperatively by x-ray measurements. Once the optimal midline position is obtained it is secured there with small plates and screws.
While repositioning the lower end of the chin bone is a logical approach, it is not a perfect procedure. While the center of the chin bone may line up with the dental and facial midlines, there remains irregular bone contours to each side. The shift will cause a inferior border protrusion on the side towards the shift and a step-off on the sides away from the shift. The relevance of these inferior border irregularities depends on the amount of horizontal bone shift. This often prominent border reductions and deficient border augmentations with the lateral sliding genioplasty.
Dr. Barry Eppley
Indianapolis, Indiana