

Migraine surgery has become popular for the few select headache patients who fulfill specific selection criteria. Having reproducible headache symptoms that correlate to specific cranial nerve locations makes the concept of nerve decompression potentially successful. Based on the premise the nerve is being pinched as the initiator of the headache attacks serves as the biologic basis for the surgery.
One of the most nerve sites treated in migraine surgery is that of the greater occipital nerve. Known to be a major contributing factor in occipital neuralgia (cervicogenic headaches), it is a spinal nerve from the 2nd cervical spinal nerve. It emerges from between the first and second cervical vertebrae up through the deep neck musculature through the trapezius muscle and fascia to innervate the skin of the back and top of the scalp. It can become entrapped as it passes through the muscle and fascia.
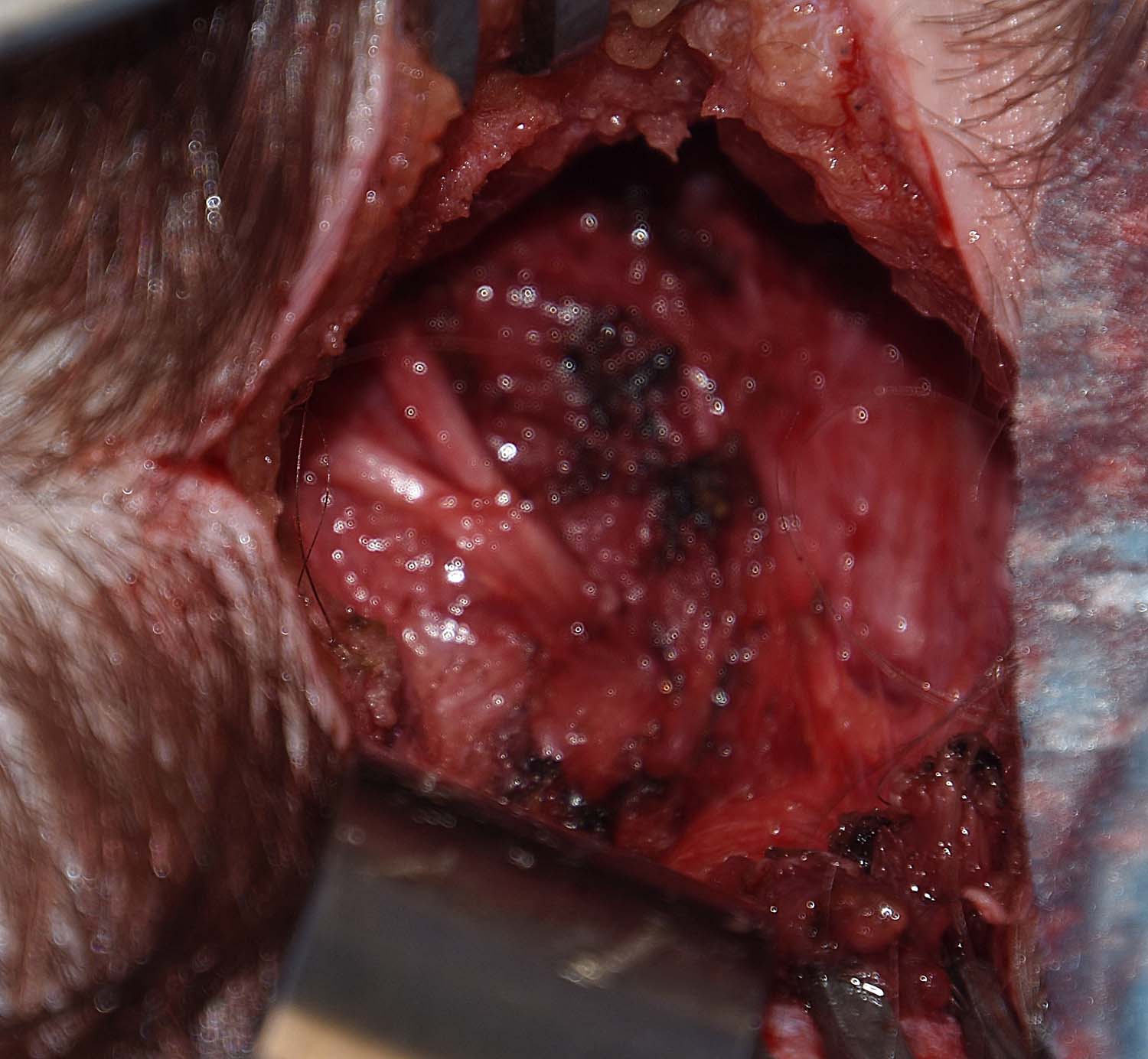 Greater occipital nerve decompression is done through a midline incision at the low end of the occipital hairline. Dissection is done through the thick layer of subcutaneous fat down to the trapezius fascia. The fascia is opened in the midline and the nerve is dissected out from the underlying muscles. Once identified the nerve is traced deep and all surrounding muscle released. It is similarly traced up toward the scalp again removing muscle as well as a fascial release along the nuchal ridge.
Greater occipital nerve decompression is done through a midline incision at the low end of the occipital hairline. Dissection is done through the thick layer of subcutaneous fat down to the trapezius fascia. The fascia is opened in the midline and the nerve is dissected out from the underlying muscles. Once identified the nerve is traced deep and all surrounding muscle released. It is similarly traced up toward the scalp again removing muscle as well as a fascial release along the nuchal ridge.
The greater occipital nerve is a big nerve whose course through the muscle and fascia gives it plenty of opportunity to be compressed or squeezed by the surrounding tissues. Its surgical decompression is associated with no adverse sequalae other than how effective it is in creating symptom relief. In my migraine surgery experience the vast majority of carefully selected occipital neuralgia patients get improvement in their symptoms, often substantially so.
Dr. Barry Eppley
Indianapolis, Indiana