

Cartilage grafting to the nose is most commonly done using anatomically convenient graft sites. This usually means the septum which offers straight graft dimensions or the ear which offer curved or shaped grafts. For many traditional rhinoplasty surgeries these graft sites are sufficient both in size and shape.
But in rhinoplasties that require larger amounts of augmentation, almost always that of the dorm, facial graft sites are too small in volume and do not have the right shape. This is where rib graft harvesting does into play if one wants avoid an implant or a cadaveric cartilage source.
While rib grafts in rhinoplasty offer plenty of volume, they usually have some shape issues. Occasionally a rib graft may actually be harvested that is straight or it can be carved to be straight. But rib graft carving must take into consideration the perichondrial lining and the ever present risk of postoperative warping.
A well known technique of avoiding rib graft warping in rhinoplasty is to change it from a solid graft to a particulated one. By dicing the rib graft into very small pieces or cubes and containing it in some form of a wrap, a very moldable cartilage graft is obtained. The debate in the use of diced rib grafts is whether it should be wrapped in autologous fascia, a very thin piece of allogeneic dermis or a bovine collagen mesh wrap (Surgicel) There is no standard consensus on the ideal wrap material.
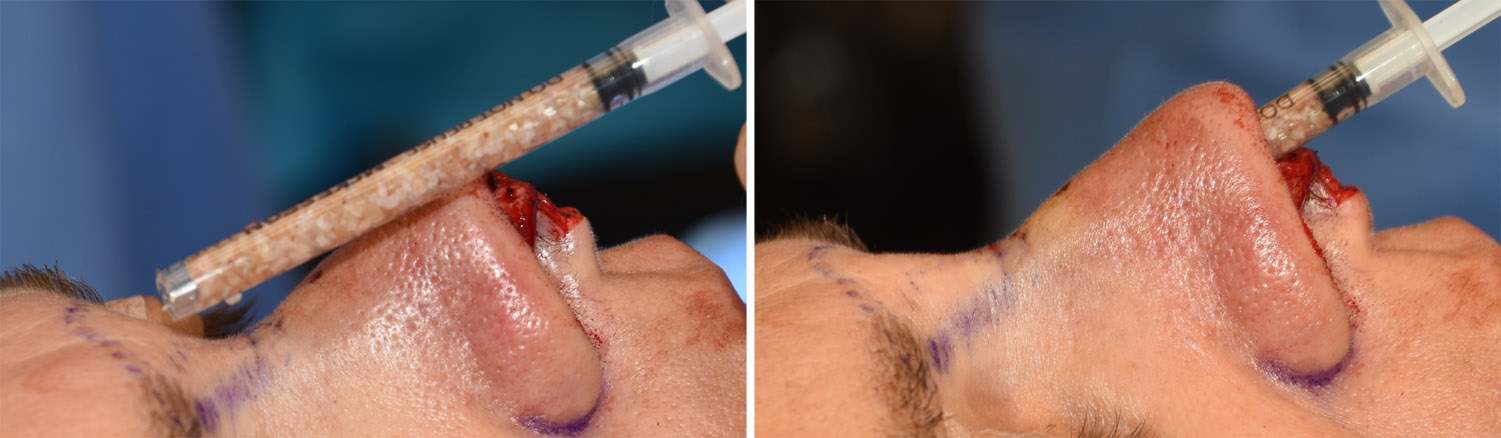 Another method to place the diced rib cartilage graft is to not wrap it at all. The placement/containment method is a small syringe from which it can be injected. This requires a precise soft tissue pocket over the dorsum and can be done through either an open or closed rhinoplasty. The diced graft is injected and then digitally molded into the desired shape. Tapes and a metal splint are placed over it to help maintain its shape.
Another method to place the diced rib cartilage graft is to not wrap it at all. The placement/containment method is a small syringe from which it can be injected. This requires a precise soft tissue pocket over the dorsum and can be done through either an open or closed rhinoplasty. The diced graft is injected and then digitally molded into the desired shape. Tapes and a metal splint are placed over it to help maintain its shape.
This injectable rhinoplasty technique allows for rapid tissue ingrowth into the diced cartilage graft. Within a few weeks it becomes very firm and maintains its shape. My and other clinical experiences show that significant graft resorption does not occur.
Dr. Barry Eppley
Indianapolis, Indiana