

Rib removal can be done for a variety of aesthetic and medical purposes. The most common aesthetic reason is for horizontal waistline narrowing with the subtotal resection of the truly free floating ribs. (#s 11 and 12) Through a small obliquely oriented skin incision on the back the midportion of the ribs are identified just lateral to the erector spine muscle and cut. From that position the rib is then dissected out to its cartilaginous tip and removed.
One of the keys to rib dissection is that it is done in a subperiosteal plane. The periosteum is tightly wrapped in a circumferential manner around the bony rib. Getting under this tissue layer allows for the smoothest and cleanest plane of dissection but also preserves all surrounding structures. This is most relevant to the neurovascular bundle that sits in a groove on the inferior side of the rib. Elevating and preserving the artery and vein makes not only for less intraoperative bleeding but prevents inadvertent nerve injury/transection and the potential for chronic postoperative rib pain.
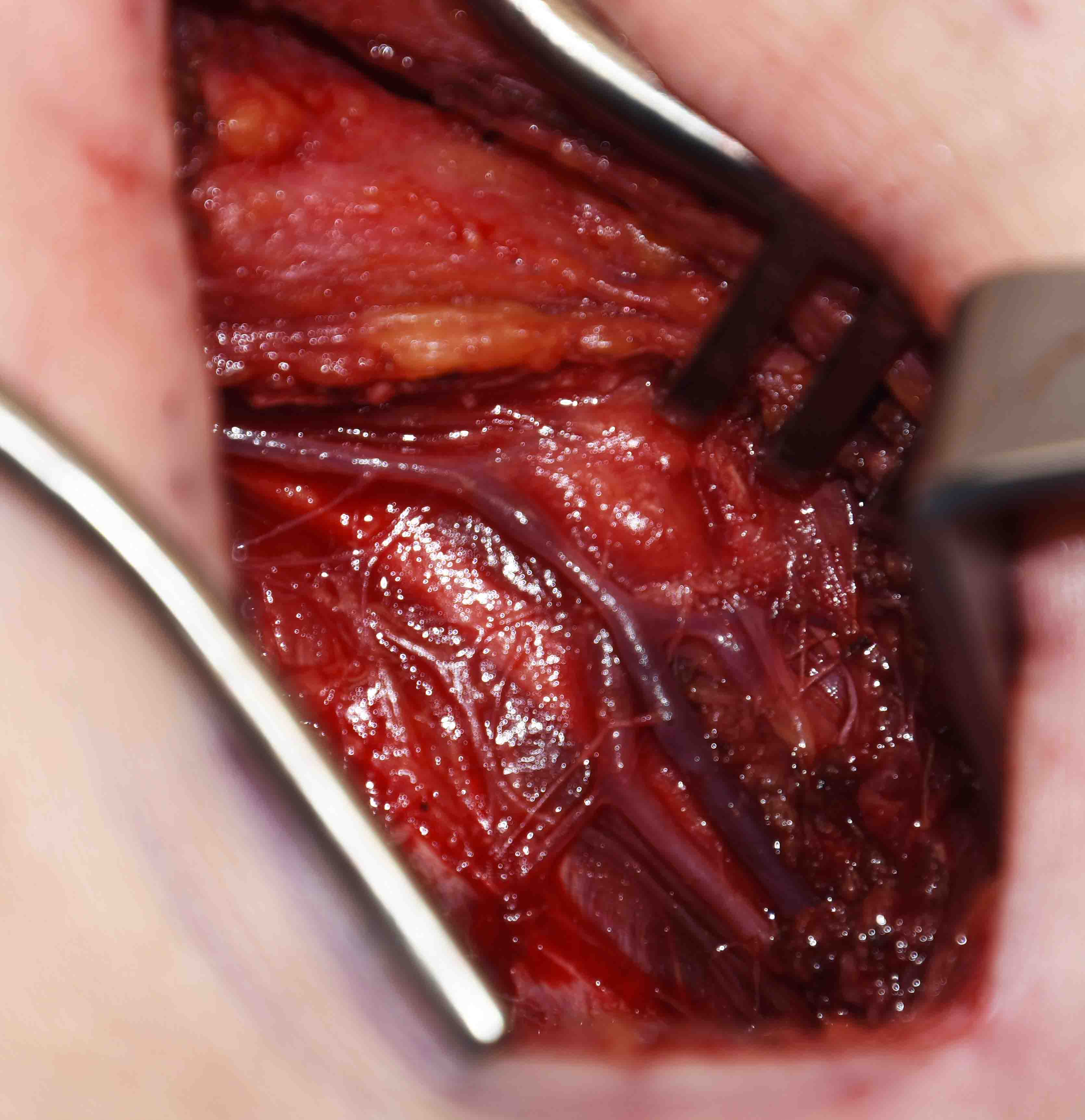 The subperiosteal rib plane of dissection is easiest on its superior aspect and harder to get out the neuromuscular bundle from its inferior bony groove. But the same instruments that are used to dissect the mucoperichondrium from the nasal septum are used to get the neuromuscular bundle out of its bony groove. Once started more proximal it is much easier to elevate out to the cartilaginous end of the rib. Once the rib is removed the vessels and nerve should be seen intact in the periosteal soft tissue cuff.
The subperiosteal rib plane of dissection is easiest on its superior aspect and harder to get out the neuromuscular bundle from its inferior bony groove. But the same instruments that are used to dissect the mucoperichondrium from the nasal septum are used to get the neuromuscular bundle out of its bony groove. Once started more proximal it is much easier to elevate out to the cartilaginous end of the rib. Once the rib is removed the vessels and nerve should be seen intact in the periosteal soft tissue cuff.
Rib removal is often associated with a destructive and very invasive surgery, undoubtably influenced by thoracic surgery which has a different intent for its performance. From an aesthetic stand point it is important that rib removal be doing through small incisions and minimize any risk for chronic postoperative pain from intercostal nerve injuries.
Dr. Barry Eppley
Indianapolis, Indiana