


Aesthetic augmentation of the posterior jawline consists of various implant options to overlay the bony jaw angle or mandibular ramus. The submuscular placement of the implant on the bone is the logical placement as the goal is to increase the size and shape of the bone. While this is a very effective technique it is not without complications…one of which directly works against the goal of a jaw angle implant.

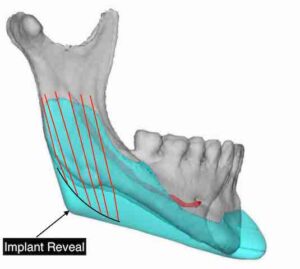 One of the two known aesthetic complications of jaw angle implants presents as a loss of adequate soft tissue (muscle) coverage over the triangular jaw angle region. This could be due to masseteric muscle dehiscence (most common) or a jaw angle implant design that extends more posterior than the natural muscle shape can stretch over it. (implant reveal) Either way, rather than having a full or more defined jaw angle region, it appears as a triangular contour deformity of various sizes that becomes most evident when chewing or biting down. But it often appears in lesser degrees even when at rest.
One of the two known aesthetic complications of jaw angle implants presents as a loss of adequate soft tissue (muscle) coverage over the triangular jaw angle region. This could be due to masseteric muscle dehiscence (most common) or a jaw angle implant design that extends more posterior than the natural muscle shape can stretch over it. (implant reveal) Either way, rather than having a full or more defined jaw angle region, it appears as a triangular contour deformity of various sizes that becomes most evident when chewing or biting down. But it often appears in lesser degrees even when at rest.
There are a variety of methods to treat this aesthetic type of jaw angle soft tissue deficiency of which the most common are injectable fillers and fat. Besides the temporary effect of synthetic fillers and the unpredictability of injected fat retention, surgical efforts to try and bring the muscle back over the implant rarely. work…and leave neck scars in the process to try and do so.

 The remaining treatment option is soft tissue implants and grafts as more assured volumetric additions. These are placed on top of the muscle rather than under it. Because it is a soft tissue augmentation method it is important that whatever material is used that it is soft and pliable. I have used Alloderm dermal grafts as well as ePTFE sheets, both of which are acceptable in smaller soft tissue jaw angle deficiencies. They can be placed through small direct (jaw angle) or indirect (earlobe) incisions.
The remaining treatment option is soft tissue implants and grafts as more assured volumetric additions. These are placed on top of the muscle rather than under it. Because it is a soft tissue augmentation method it is important that whatever material is used that it is soft and pliable. I have used Alloderm dermal grafts as well as ePTFE sheets, both of which are acceptable in smaller soft tissue jaw angle deficiencies. They can be placed through small direct (jaw angle) or indirect (earlobe) incisions.

 But in larger surface area or deeper jaw angle soft tissue contour deformities I have found that ultrasoft solid silicone shaped implants are most effective. Their elastic deformation properties make them easy to insert through small skin incisions. They offer obvious volume permanence. It may seem at odds to have correct a hard tissue implant-related problem with a soft tissue implant but that only seems that way because it has been so rarely done.
But in larger surface area or deeper jaw angle soft tissue contour deformities I have found that ultrasoft solid silicone shaped implants are most effective. Their elastic deformation properties make them easy to insert through small skin incisions. They offer obvious volume permanence. It may seem at odds to have correct a hard tissue implant-related problem with a soft tissue implant but that only seems that way because it has been so rarely done.
The implant is usually custom designed based on the outline of the external soft tissue contour deformity and an estimate of how much thickness is needed. The greatest thickness is located over the jaw angle region and feathers out to the posterior, superior and anterior ends. If it exists on both sides it often has different shapes between the two sides.

 The placement of ultrasoft silicone jaw angle soft tissue implants, like Alloderm and ePTFE, can be placed through a 1 cm direct incision or from one around the earlobe. In men int particular the beard skin heals so well that the direct approach is preferred. A subcutaneous skin flap is raised with facelift scissors mainly the created pocket no bigger than the external skin marks. The implant can have perfusion holes placed if desired, which I prefer to usually do to allow for tissue ingrowth and soft tissue intraimplant fixation.
The placement of ultrasoft silicone jaw angle soft tissue implants, like Alloderm and ePTFE, can be placed through a 1 cm direct incision or from one around the earlobe. In men int particular the beard skin heals so well that the direct approach is preferred. A subcutaneous skin flap is raised with facelift scissors mainly the created pocket no bigger than the external skin marks. The implant can have perfusion holes placed if desired, which I prefer to usually do to allow for tissue ingrowth and soft tissue intraimplant fixation.
 Getting the implant into good position is obviously a key step and is best aided by the small incision at the back end of the jaw angle area. If the pocket is not overextended implant introduction into the pocket is all that is needed. Suture fixation to the muscle can also be done if desired. Closure of the skin incision is done in two layers with small resorbable sutures.
Getting the implant into good position is obviously a key step and is best aided by the small incision at the back end of the jaw angle area. If the pocket is not overextended implant introduction into the pocket is all that is needed. Suture fixation to the muscle can also be done if desired. Closure of the skin incision is done in two layers with small resorbable sutures.
 These soft tissue jaw angle implants are very effective at addressing iatrogenic-induced soft tissue contour deformities after jaw angle or jawline implant placements. Their success makes me wonder that they may also have a role int the primary jaw angle implant patient who is only seeking a a very modest augmentation effect. Sort of intermediary option between injectable fillers and submuscular placed implants.
These soft tissue jaw angle implants are very effective at addressing iatrogenic-induced soft tissue contour deformities after jaw angle or jawline implant placements. Their success makes me wonder that they may also have a role int the primary jaw angle implant patient who is only seeking a a very modest augmentation effect. Sort of intermediary option between injectable fillers and submuscular placed implants.
Dr. Barry Eppley
Indianapolis, Indiana