

Breast augmentation is one of the most popular body contouring operations. It creates an instantaneous effect that often can cause quite a dramatic change in a woman’s chest appearance. But its effects are due to a medical device and, as such, makes it prone to a higher rate of complications than any plastic surgery operation where natural tissue is used to create the aesthetic improvement.
 This one simple and obvious fact, the need for a synthetic implant, in breast augmentation is frequently overlooked by patients as they understandably focus on the upcoming positive changes. No patient ever thinks that they will actually be the one who suffers a complication or has to have revision surgery for a more optimal result.
This one simple and obvious fact, the need for a synthetic implant, in breast augmentation is frequently overlooked by patients as they understandably focus on the upcoming positive changes. No patient ever thinks that they will actually be the one who suffers a complication or has to have revision surgery for a more optimal result.
While there are a variety of potential complications in breast augmentation surgery, the most common is implant or breast mound asymmetry. While each individual augmented breast mound may look fine in its own right, the paired nature of the breasts and their close proximity make symmetry of the result of critical aesthetic importance.
Over the years and after many breast augmentation procedures, I have observed numerous important issues that can influence the likelihood of this after surgery problem. Some of these can be influenced by decisions made before and during surgery, while others are beyond the surgeon’s control. Here are my insights into this undesired outcome of breast augmentation surgery and how best to avoid them.
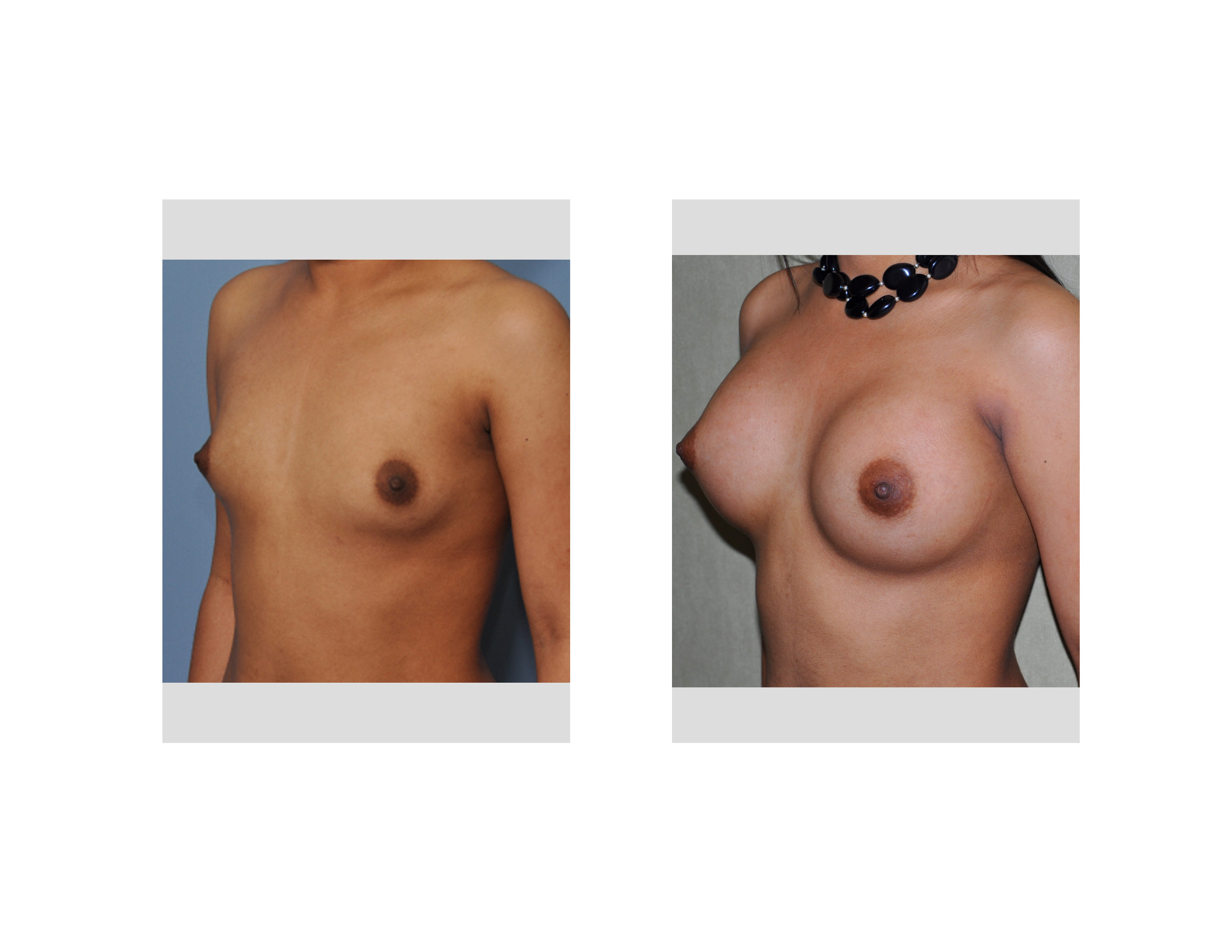
 IMPLANT SIZE While many plastic surgeons make every effort to accommodate patient requests for the breast size they want, woman often do not understand the consequences of their choices. When the implant size potentially exceeds the ability of the breast tissues to support them, asymmetry, bottoming out and implant displacement is more likely to occur. What constitutes adequate tissue support is defined by the breast base width and the quality of the overlying breast tissues. But one of the key factors is the location of the inframammary fold, the tight restraining line of the lower breast mound. When it has to be dropped down to accommodate the implant size, which is often needed, the risk of implant asymmetry is increased.The size and weight of the implant may make it drop down lower than desired later. Or inadequate release of the fold or scar tissue formation later may make the implant sit higher than desired. The point being…the bigger the implant the higher the risk.
IMPLANT SIZE While many plastic surgeons make every effort to accommodate patient requests for the breast size they want, woman often do not understand the consequences of their choices. When the implant size potentially exceeds the ability of the breast tissues to support them, asymmetry, bottoming out and implant displacement is more likely to occur. What constitutes adequate tissue support is defined by the breast base width and the quality of the overlying breast tissues. But one of the key factors is the location of the inframammary fold, the tight restraining line of the lower breast mound. When it has to be dropped down to accommodate the implant size, which is often needed, the risk of implant asymmetry is increased.The size and weight of the implant may make it drop down lower than desired later. Or inadequate release of the fold or scar tissue formation later may make the implant sit higher than desired. The point being…the bigger the implant the higher the risk.
INCISION LOCATION There are four incisions in and around the breast mound that can be used to insert an implant. While in theory they are just a way to get into the breast mound to do the identical thing (develop the implant pocket), they are more than just ‘a way to get there’. While patients understandably focus on the size of the incision, surgeons are more interested in the ability to adequately make a breast pocket through them. The best incision to do so is through a lower breast fold or inframammary fold incision. (technically usually lower) This incision provides direct access to the critical fold area and the lower attachments of the pectoralis major muscle, both issues which highly influence the final position of the implant. Other incisions do work but they all have higher risks of implant positioning problems due to lack of visibility of this area or the easy access to manipulate it.
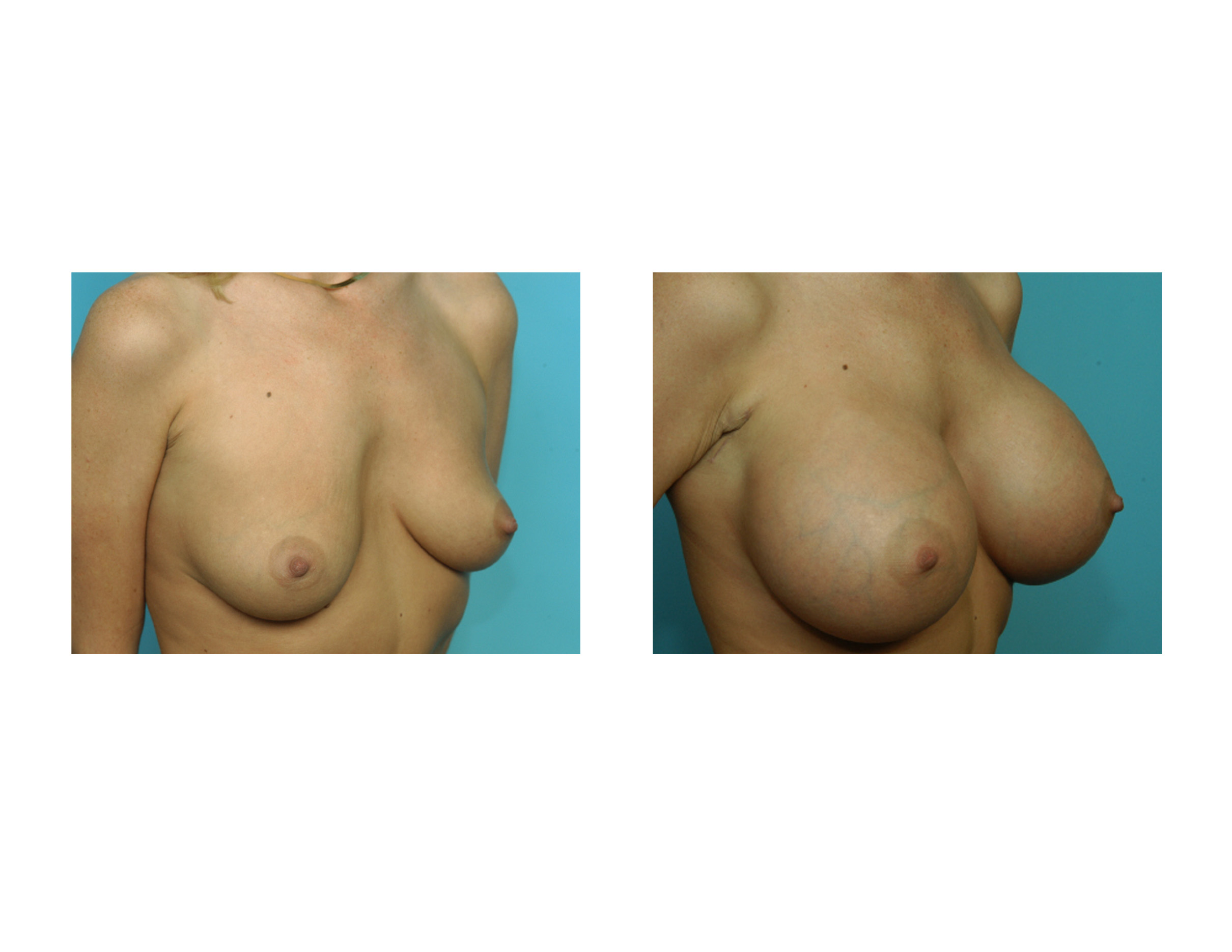
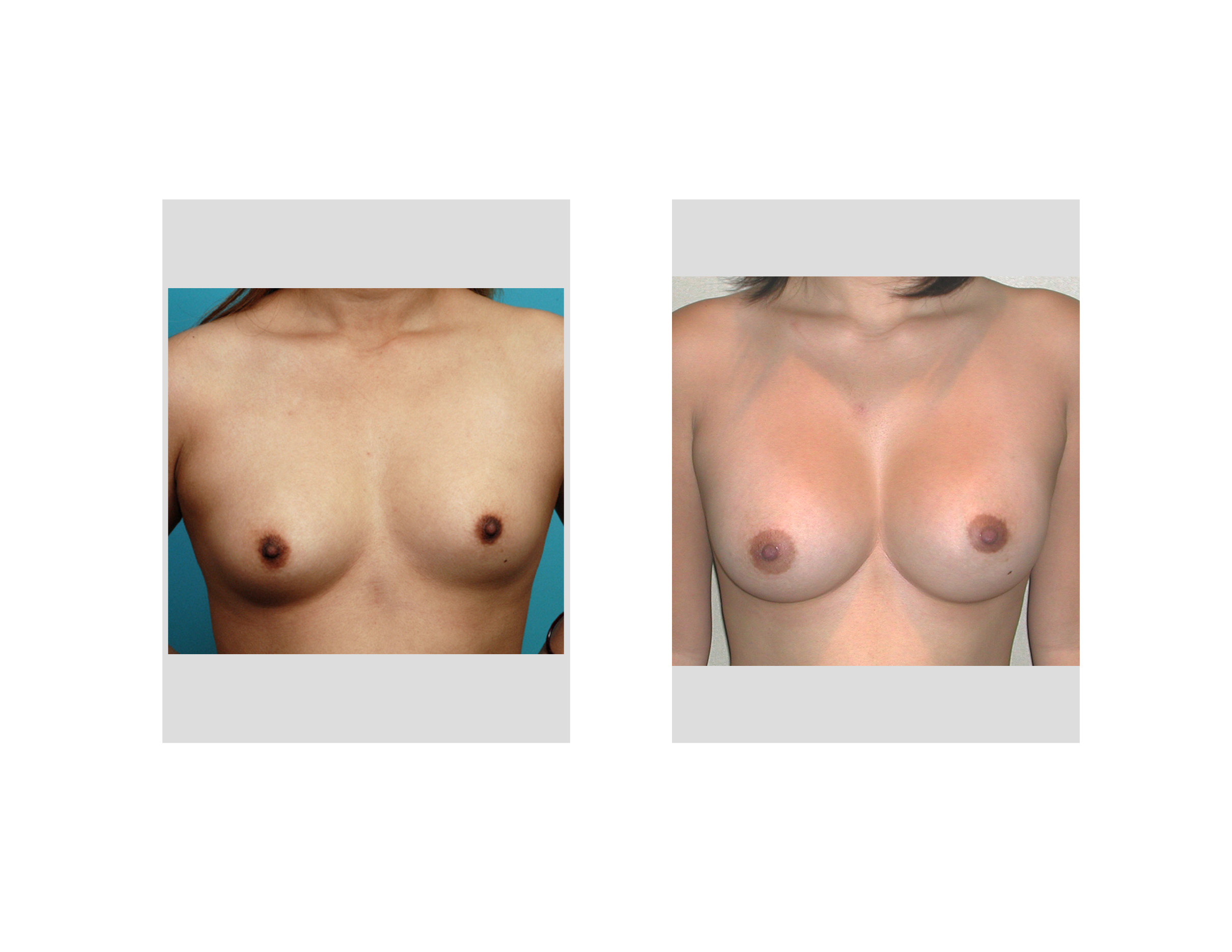 BREAST ASYMMETRY Few women have perfect natural breast symmetry. One may think they do when the breasts are small, but when inflated with implants to a much larger size, even subtle amounts of breast asymmetry become magnified. As the old plastic surgery saying goes ‘they are sisters, not twins’. Breast asymmetry poses problems for ideal breast augmentation results in both the shape of the mounds and in the position of the nipples. Different sized implants in each breast and small nipple adjustments may help but most breast asymmetries can only be improved and not ‘cured’. One should next expect perfection in their breasts unless they were perfect from the start.
BREAST ASYMMETRY Few women have perfect natural breast symmetry. One may think they do when the breasts are small, but when inflated with implants to a much larger size, even subtle amounts of breast asymmetry become magnified. As the old plastic surgery saying goes ‘they are sisters, not twins’. Breast asymmetry poses problems for ideal breast augmentation results in both the shape of the mounds and in the position of the nipples. Different sized implants in each breast and small nipple adjustments may help but most breast asymmetries can only be improved and not ‘cured’. One should next expect perfection in their breasts unless they were perfect from the start.
BREAST SAGGING Large amounts of breast sagging require the concomitant use of some form of a breast lift with an implant to get the desired result. But smaller amounts of sagging may make one think that implant augmentation will lift and even them out. The desire to avoid scars on the breast mound is understandable and may in some cases even work. But in other cases the placement of breast implants may merely prove that adjustment of the overlying breast tissues with scars may be needed. It is important to be realistic as to what implants can do in the face of loose breast skin and a low nipple position. Avoid trying to use large implants to overcome breast sagging that a breast lift is better suited to do.
REVISIONAL SURGERY When one breast is higher or lower than the other side after augmentation surgery, a revision will be needed to help make them more symmetric. But it is important to not jump to early to have a revision and be patient with the settling process. This is usually a minimum of three to six months after surgery. Impatience can lead to ‘chasing a moving target’ which is a set up for additional revisional surgery needs. There is also the judgment of when one should have a revision at all. Every surgery has risks of infection and causing scar and capsular contracture problems. Very small differences in implant positions make should give one pause about aiming for ideal symmetry. As the old plastic surgery axiom goes ‘the enemy of good is, if fact, perfection’.
Dr. Barry Eppley
Indianapolis, Indiana