

Removal of parts of ribs for body contouring is most commonly associated with waistline narrowing. This relates specifically to the lower ribs, the so called floating ribs (#11 and 12), although in my technique I remove part of rib #10 as well. While this posterior ribcage area is the common aesthetic rib removal area, an anterior location exists as well.
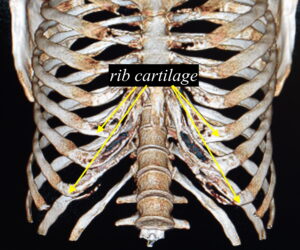 The prominent part of the anterior ribcage is known as the subcostal margin. This rib area can stick out on one side or both creating an undesired protrusion. In some women the subcostal rib margin may stick out further than that of their natural breast development. Unlike the posterior ribs which have their effect on the waistline because of their length, the subcostal margin has a looped configuration consisting of bone and cartilage. How these two rib components come together and their angulation in so doing can create a prominent subcostal rib margin.
The prominent part of the anterior ribcage is known as the subcostal margin. This rib area can stick out on one side or both creating an undesired protrusion. In some women the subcostal rib margin may stick out further than that of their natural breast development. Unlike the posterior ribs which have their effect on the waistline because of their length, the subcostal margin has a looped configuration consisting of bone and cartilage. How these two rib components come together and their angulation in so doing can create a prominent subcostal rib margin.
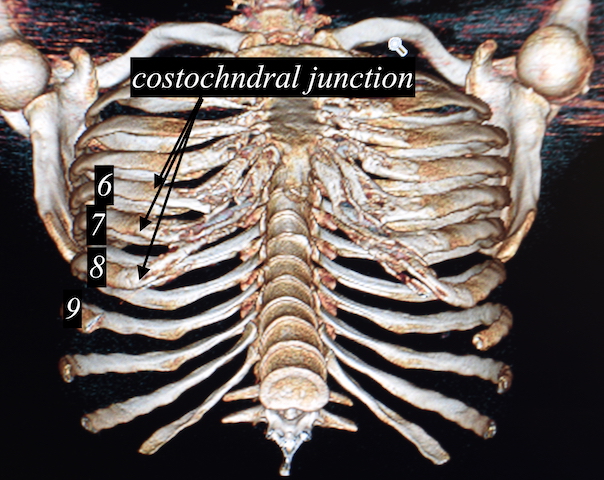
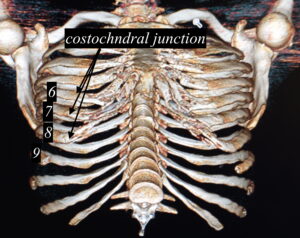 The subcostal margin is primarily composed of rib #8 in most people. The cartilaginous portion of rib #9, which comes in just below #8 can also contribute to the subcostal protrusion. In some cases it may even involve rib #10 which has a shorter cartilage end and is not connected to rib #9 above it,. As a result much of subcostal rib margin reduction is cartilaginous unlike posterior rib removal of #10, 11 and 12 which is all bone.
The subcostal margin is primarily composed of rib #8 in most people. The cartilaginous portion of rib #9, which comes in just below #8 can also contribute to the subcostal protrusion. In some cases it may even involve rib #10 which has a shorter cartilage end and is not connected to rib #9 above it,. As a result much of subcostal rib margin reduction is cartilaginous unlike posterior rib removal of #10, 11 and 12 which is all bone.
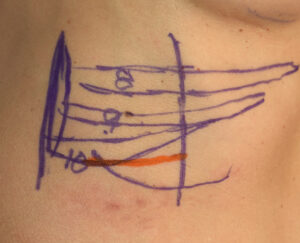

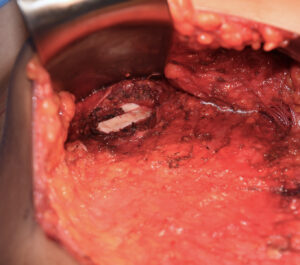
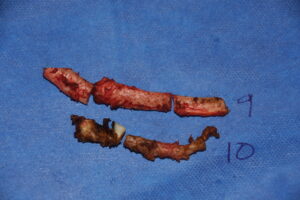 In reducing a prominent subcostal margin it is necessary to consider cartilage removals of either ribs 8, 9, and 10 through a direct incision. It could be one, two or all three that need to be reduced depending on the prominence and its shape. Because these are all cartilage such ribs can be reduced/removed by shaving. Only in older patients would a high speed burring technique be needed where the cartilages are stiffer due to being partially calcified.
In reducing a prominent subcostal margin it is necessary to consider cartilage removals of either ribs 8, 9, and 10 through a direct incision. It could be one, two or all three that need to be reduced depending on the prominence and its shape. Because these are all cartilage such ribs can be reduced/removed by shaving. Only in older patients would a high speed burring technique be needed where the cartilages are stiffer due to being partially calcified.

 The discomfort associated with subcostal rib removal is less than with the posterior ribs because they are covered under less muscle. The rectus abdomens muscle must still be traversed but this is best done by sweeping the muscle medially rather than cutting through it.
The discomfort associated with subcostal rib removal is less than with the posterior ribs because they are covered under less muscle. The rectus abdomens muscle must still be traversed but this is best done by sweeping the muscle medially rather than cutting through it.

 The biggest consideration in subcostal rib removal is not whether it is effective but whether the scar associated with it is a worthy tradeoff. The scar is not in any hidden location or in a natural skin crease so this must be considered. It is also not possible to access the subcostal margin through an inframammary incisional approach as it is simply to far away to be effective. (I have tried with minimal success)
The biggest consideration in subcostal rib removal is not whether it is effective but whether the scar associated with it is a worthy tradeoff. The scar is not in any hidden location or in a natural skin crease so this must be considered. It is also not possible to access the subcostal margin through an inframammary incisional approach as it is simply to far away to be effective. (I have tried with minimal success)
 There are rare cases of subcostal rib removal which can be done in scarless manner through a tummy tuck approach. But this requires that one also needs a tummy tuck as well and is not done just for the incisional access alone.
There are rare cases of subcostal rib removal which can be done in scarless manner through a tummy tuck approach. But this requires that one also needs a tummy tuck as well and is not done just for the incisional access alone.
Dr. Barry Eppley
Indianapolis, Indiana