


Introduction
Subcostal rib flare refers to a visible or palpable outward angulation of the lower ribs—typically ribs 7 through 10—along the subcostal margin where the rib cage meets the upper abdomen. It is most commonly perceived as a protrusion beneath the chest, particularly when viewed from the front or side.
Clinical Appearance
Patients often describe a firm, asymmetric, or symmetric prominence beneath the lower chest that may be noticeable at rest or under clothing.
Common Causes
- Chest wall anatomy and skeletal shape
Normal anatomic variation, pectus excavatum, or pectus carinatum - Posture and muscular imbalance
Tight diaphragm, weak abdominal or core musculature - Spinal alignment disorders
Scoliosis or other axial deviations - Respiratory mechanics
Chronic upper-chest breathing patterns - Prior surgery or trauma
Less common, but possible contributing factors
Why It Matters
- Aesthetic concerns
Visible prominence or asymmetry beneath clothing - Functional considerations
Occasionally associated with poor core stability or inefficient breathing mechanics
Evaluation
- Physical examination (standing and supine)
- Postural assessment
- Imaging (X-ray or CT) only when a structural abnormality is suspected or surgical intervention is being considered
Management Options
Initial management may include postural correction, physical therapy, and breathing or core-strengthening programs. When these approaches are ineffective or inappropriate, surgical correction through direct rib modification represents the definitive option.
Case Study
A young, petite female presented with concern over symmetric subcostal rib flare. She had previously undergone rib removal surgery for waist contouring and was not averse to additional scarring.

 Under general anesthesia, abdominal liposuction was first performed, including fat reduction over the subcostal margins. Bilateral anterior subcostal incisions were then made. The rectus abdominis muscle was split vertically to allow access to the underlying ribs. The cartilaginous ends of ribs 9 and 10 were removed, and rib 8 was contoured by shaving.
Under general anesthesia, abdominal liposuction was first performed, including fat reduction over the subcostal margins. Bilateral anterior subcostal incisions were then made. The rectus abdominis muscle was split vertically to allow access to the underlying ribs. The cartilaginous ends of ribs 9 and 10 were removed, and rib 8 was contoured by shaving.

 The rectus abdominus muscle was reapproximated, and the skin was closed using a subcuticular technique. A marked reduction in subcostal protrusion was immediately evident.
The rectus abdominus muscle was reapproximated, and the skin was closed using a subcuticular technique. A marked reduction in subcostal protrusion was immediately evident.
Discussion
Cosmetic surgical correction of rib flare is uncommon and must be selectively applied. However, surgical options do exist for patients with prominent, symptomatic rib flare or when it contributes to a broader torso contour deformity.
Goals of Rib Flare Surgery
The objective is to reduce outward projection of the costal margin to improve torso contour—not to alter rib function or pulmonary mechanics.
Surgical Options
Surgical approaches range from indirect correction during abdominal contouring procedures to direct costal margin modification. While indirect methods preserve rib structure, they tend to have limited effectiveness, particularly in cases of significant subcostal protrusion.
The two most effective techniques are rib remodeling and rib resection.
1. Rib Remodeling (RibXcar)
 This technique involves scoring the anterior costal cartilages (typically ribs 8–10) with controlled bending or fracturing to reposition them inward.
This technique involves scoring the anterior costal cartilages (typically ribs 8–10) with controlled bending or fracturing to reposition them inward.
Key Features
- Requires prolonged postoperative compression or banding for several months
- Relies on cartilage and fibrous healing to maintain correction
Indications
- Severe or rigid rib flare
- Significant asymmetry
- Failure of conservative or indirect measures
Limitations and Risks
- Incomplete or temporary correction
- Risk of relapse over time
?? Importantly, failure of RibXcar does not preclude secondary rib resection.
2. Rib Resection
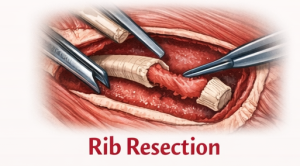 This approach involves open resection or shaving of the flared cartilaginous rib segments.
This approach involves open resection or shaving of the flared cartilaginous rib segments.
Technical Considerations
- Vertical splitting (not transverse cutting) of the rectus abdominis muscle is required
- Surgical drains are usually unnecessary
Indications
- Structurally significant rib flare rather than postural prominence
- Rib flare more pronounced when supine than standing
- Marked asymmetry
- Acceptance of bilateral visible subcostal scars
Risks
- Permanent subcostal scarring
- Incomplete correction
- Potential visibility or palpability of rib margins
Choosing the Appropriate Procedure
The decision to pursue RibXcar versus proceeding directly to rib resection depends primarily on scar tolerance and the severity of the rib flare.
- Patients seeking to avoid visible scars and who have mild to moderate rib flare may find RibXcar an acceptable option, provided they understand its limitations.
- Patients willing to accept subcostal scars in exchange for more predictable and durable results—and who have more severe rib flare—are better candidates for rib resection.
Key Points
- Subcostal rib flare consists of submuscular cartilaginous prominences at the junction of the lower rib cage and upper abdomen.
- Surgical correction options include cartilage reshaping via percutaneous chondrotomies (RibXcar) or open cartilage resection.
- Each technique has distinct advantages and limitations that must be considered based on rib flare severity and patient motivation for correction.
Barry Eppley, MD, DMD
World-Renowned Plastic Surgeon