


Background
Aesthetic lip augmentation can be achieved through a variety of methods. Injectable fillers remain the most commonly performed option; however, they are not suitable for all patients, particularly those with unfavorable natural lip anatomy or those who prefer a permanent solution. For these patients, surgical techniques provide durable results through direct lip reshaping or procedures performed in adjacent regions.
Among surgical options, the subnasal (“bullhorn”) upper lip lift is the most widely recognized. It is effective because the incision is concealed at the nasal base, away from the lip itself. Nonetheless, it does not provide a complete reshaping of the upper lip. Specifically, it does not address the outer third of the lip or the oral commissures. Therefore, careful preoperative analysis is required to evaluate lateral vermilion show. In patients with limited lateral vermilion, a subnasal lip lift alone risks creating an A-frame deformity. In such cases, combining the procedure with lateral vermilion advancements can convert it into a comprehensive upper lip reshaping approach.
The lower lip presents unique challenges. Unlike the upper lip, it lacks a defined central landmark, and no nearby structures provide favorable scar concealment. For full lower lip augmentation, a vermilion advancement from commissure to commissure is reliable. However, when minimizing external scarring is a priority, a central V-Y mucosal advancement performed intraorally is an alternative. This technique everts the central lower lip and, when combined with lateral vermilion advancements, creates a complete augmentation. Typically, the lower lip requires less augmentation than the upper, as it is naturally fuller in most patients.
Case Study
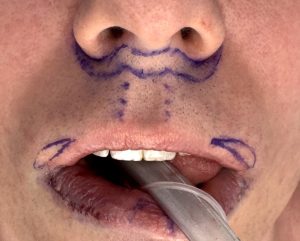
 A young male patient sought both upper and lower lip reshaping as part of a broader facial contouring plan. His upper lip measured 18 mm along the philtral columns, with a reasonably defined Cupid’s bow. Vermilion show of the upper lip diminished well before reaching the commissures. Conversely, his lower lip was naturally fuller, with vermilion extending nearly to the corners.
A young male patient sought both upper and lower lip reshaping as part of a broader facial contouring plan. His upper lip measured 18 mm along the philtral columns, with a reasonably defined Cupid’s bow. Vermilion show of the upper lip diminished well before reaching the commissures. Conversely, his lower lip was naturally fuller, with vermilion extending nearly to the corners.
The surgical plan included:
 A 5 mm subnasal lip lift, combined with lateral vermilion advancements to extend lip fullness to the commissures.
A 5 mm subnasal lip lift, combined with lateral vermilion advancements to extend lip fullness to the commissures.
- A central V-Y mucosal advancement of the lower lip, augmented by lateral vermilion advancements, to achieve proportional enhancement relative to the upper lip.
 A 5 mm subnasal lip lift, combined with lateral vermilion advancements to extend lip fullness to the commissures.
A 5 mm subnasal lip lift, combined with lateral vermilion advancements to extend lip fullness to the commissures.
 A central V-Y mucosal advancement of the lower lip, augmented by lateral vermilion advancements, to achieve proportional enhancement relative to the upper lip.
A central V-Y mucosal advancement of the lower lip, augmented by lateral vermilion advancements, to achieve proportional enhancement relative to the upper lip.Discussion
This case illustrates that comprehensive surgical lip enhancement frequently requires combining techniques tailored to the patient’s anatomy and goals. Selection of the appropriate approach depends on:
- Vermilion display across the entire lip length.
- The patient’s tolerance for external versus internal scars.
- The degree of augmentation desired.
With the exception of total vermilion advancement, no single technique provides complete lip reshaping in isolation.
Key Points
- Subnasal lip lifts may necessitate adjunctive lateral vermilion advancements to prevent A-frame deformities.
- In the lower lip, a central V-Y mucosal advancement functions as the counterpart to the subnasal lift, offering augmentation while minimizing external scars.
- Preoperative assessment must consider lateral vermilion deficiency in both lips to ensure balanced results.
Dr. Barry Eppley
World-Renowned Plastic Surgeon