


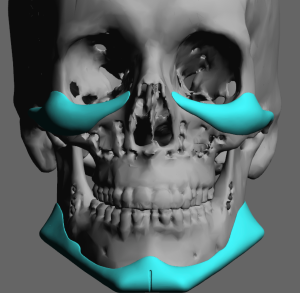
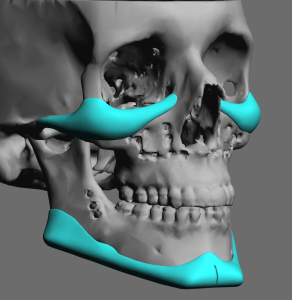
 The classic facial masculinization procedure in my practice is the combination of ‘cheek’ and ‘jaw’ implants. Technically these are more than these names imply. These male facial implants are custom made and cover larger surface areas of the midface and jawbone to create their effects. For this reason they are better described as infraorbital-malar (cheek) and total jawline (jaw) implants.
The classic facial masculinization procedure in my practice is the combination of ‘cheek’ and ‘jaw’ implants. Technically these are more than these names imply. These male facial implants are custom made and cover larger surface areas of the midface and jawbone to create their effects. For this reason they are better described as infraorbital-malar (cheek) and total jawline (jaw) implants.
 With such larger facial implants than standard implant sizes an important aspect of the surgery is the incisions used for their placement. While getting good implant placement is paramount, limiting visible incisions/scars is also an important element of the surgery. Given the size of the implants the incisional load is quite small which is helped by having two out of the five incisions needed for their placement to be intraoral.
With such larger facial implants than standard implant sizes an important aspect of the surgery is the incisions used for their placement. While getting good implant placement is paramount, limiting visible incisions/scars is also an important element of the surgery. Given the size of the implants the incisional load is quite small which is helped by having two out of the five incisions needed for their placement to be intraoral.

 When doing these two custom facial implant procedures together the infraorbital-malar (IOM) implants are always done first and they are the most sterile part of the procedure. For IOM implants a limited or hemi- lower blepharoplasty incision is used. This means there is a very small lateral canthal extension but the incision only crosses under the lower lash line out to the pupil of the eye. A skin muscle flap is raised down to the bone. This provides enough access to develop the full extent of the implant pocket and decreases the disruption of the orbicularis muscle. The incision length compared to the east-west length of the implant is less than a third. Once the implant is passed through the incision and positioned it is usually secured with single screw to the upper cheekbone. (and sometimes an additional screw along the infraorbital rim if needed)
When doing these two custom facial implant procedures together the infraorbital-malar (IOM) implants are always done first and they are the most sterile part of the procedure. For IOM implants a limited or hemi- lower blepharoplasty incision is used. This means there is a very small lateral canthal extension but the incision only crosses under the lower lash line out to the pupil of the eye. A skin muscle flap is raised down to the bone. This provides enough access to develop the full extent of the implant pocket and decreases the disruption of the orbicularis muscle. The incision length compared to the east-west length of the implant is less than a third. Once the implant is passed through the incision and positioned it is usually secured with single screw to the upper cheekbone. (and sometimes an additional screw along the infraorbital rim if needed)

 An IOM implant actually provides support to the lower eyelid through an upward displacement of the lid-cheek tissues. And, unlike a traditional lower blepharoplasty where tissue and support is removed/lost, the risk of lower eyelid malpositon risk is much lower as a result. The lower eyelid incision is still closed by adding suture support by a cheek suspension and canthopexy prior to skin closure.
An IOM implant actually provides support to the lower eyelid through an upward displacement of the lid-cheek tissues. And, unlike a traditional lower blepharoplasty where tissue and support is removed/lost, the risk of lower eyelid malpositon risk is much lower as a result. The lower eyelid incision is still closed by adding suture support by a cheek suspension and canthopexy prior to skin closure.
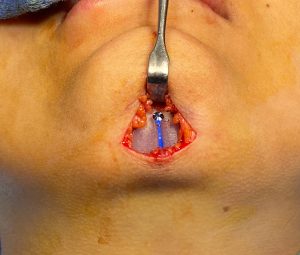
 The even larger custom jawline implant is introduced through a submental skin incision that is really not much longer than the lower eyelid incision. While some prefer a completely intraoral approach this would not be my choice given the increased risk of infection. The goal is to insert the implant through the most sterile approach possible (skin incision) and only use the necessary bilateral posterior vestibular incisions for pocket development and to aid positioning and fixation of the jaw angle portions of the implant. It is still not as sterilely placed as an IOM implant but far better than dragging an implant inside the mouth with an exclusive intraoral approach..
The even larger custom jawline implant is introduced through a submental skin incision that is really not much longer than the lower eyelid incision. While some prefer a completely intraoral approach this would not be my choice given the increased risk of infection. The goal is to insert the implant through the most sterile approach possible (skin incision) and only use the necessary bilateral posterior vestibular incisions for pocket development and to aid positioning and fixation of the jaw angle portions of the implant. It is still not as sterilely placed as an IOM implant but far better than dragging an implant inside the mouth with an exclusive intraoral approach..


 The ability to get such a long jawline implant through such a small incision is an art form based on technique and the elastic deformation properties of the implant. One side goes in at a time, passing each side under the mental nerve and back to where it can be seen through the intraoral incisions. Once positioned screw fixation is done through a percutaneous approach as this is the only way to ensure implant positioning way back onto the jaw angle bone and still get good screw fixation into it. Intraoral screw fixation is fraught with many issues due to the tight working space of the elevated masseter muscle and the bone. The key is that the screws must go to the proper implant position…not the reverse. (intraoral screw placement tends to pull the implant toward where the screws are easiest to place) All three incisions are then closed with restorable sutures with paired internal sutures with much a much slower resorption profile.
The ability to get such a long jawline implant through such a small incision is an art form based on technique and the elastic deformation properties of the implant. One side goes in at a time, passing each side under the mental nerve and back to where it can be seen through the intraoral incisions. Once positioned screw fixation is done through a percutaneous approach as this is the only way to ensure implant positioning way back onto the jaw angle bone and still get good screw fixation into it. Intraoral screw fixation is fraught with many issues due to the tight working space of the elevated masseter muscle and the bone. The key is that the screws must go to the proper implant position…not the reverse. (intraoral screw placement tends to pull the implant toward where the screws are easiest to place) All three incisions are then closed with restorable sutures with paired internal sutures with much a much slower resorption profile.
The combination of custom IOM and jawline implants enhances the most prominent horizontal convexities of the face. Their long lengths would suggest that their placement would carry a high incisional/scar burden to place. But with good surgical technique their placement can be done with remarkably low scarring risks due to the mobile window concept as well as the willingness to work within the limited confines of the entrances to the implant pockets.
Dr. Barry Eppley
World Renowned Plastic Surgeon