

Pectoral implants are the male equivalent of breast implants for women. The fundamental difference is that pectoral implants are a muscle enhancing procedure while breast implants are a non-muscular soft tissue (breast mound) enhancing procedure. These anatomic differences make for subtle but significant differences in the surgical technique in how the implants are placed.
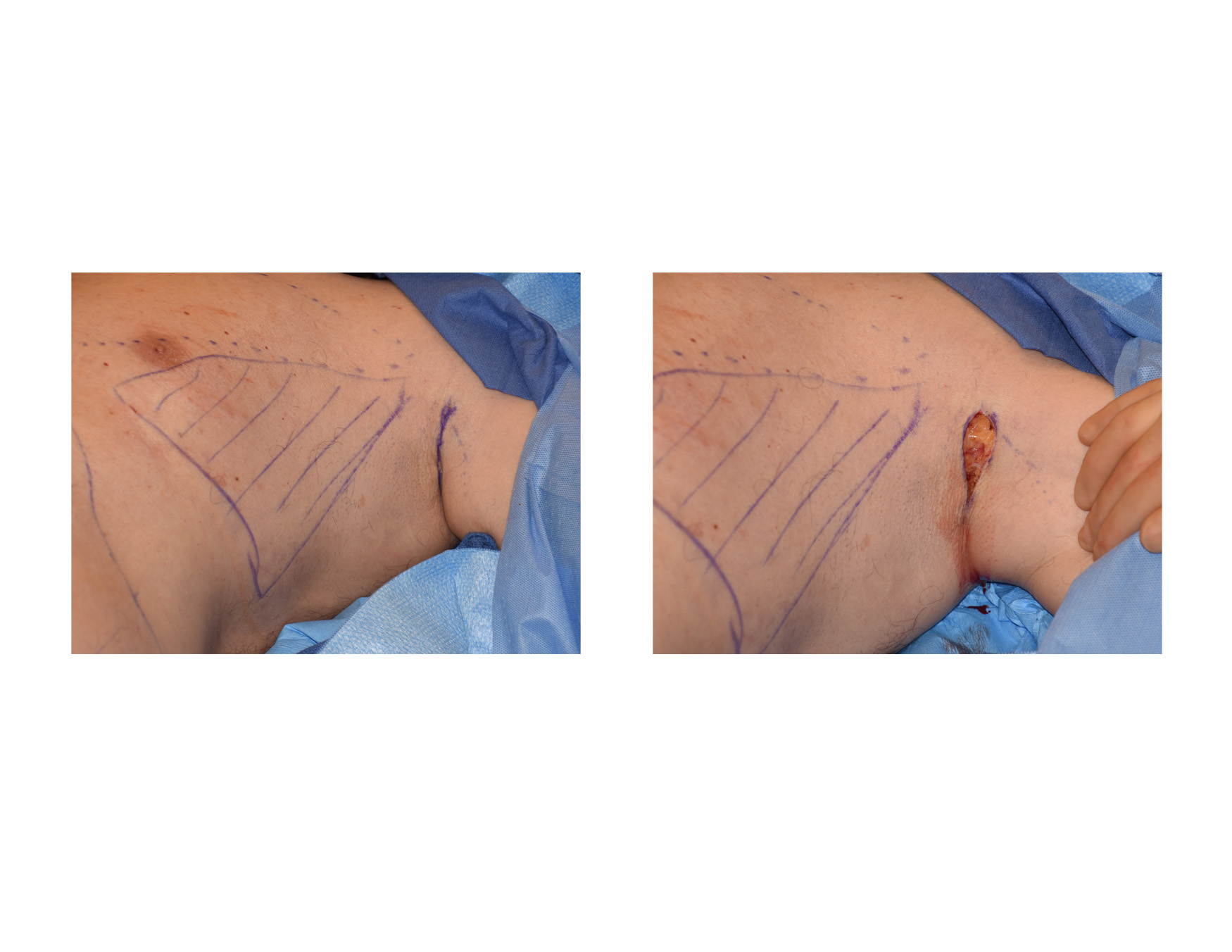
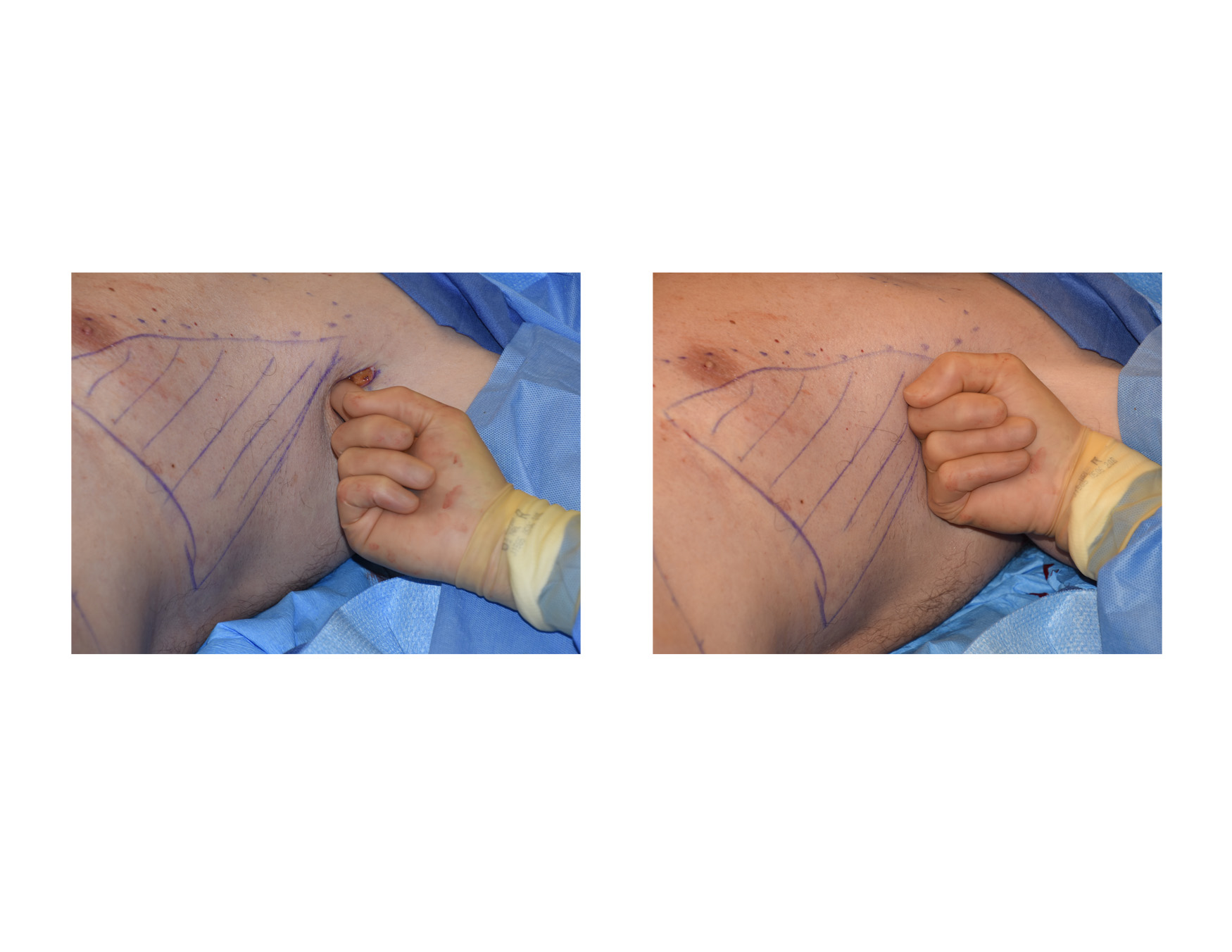 Pectoral implants are placed somewhat similarly as that of transaxillary breast augmentation. A high axillary skin incision is made that is about 6cms long in the skin crease just lateral to the edge of the pectoral muscle. Once through the skin blunt dissection with a finger is carried into the submuscular place superiorly towards the clavicle. Once the clavicle is reached the finger is turned downward sweeping across the top of the ribs.
Pectoral implants are placed somewhat similarly as that of transaxillary breast augmentation. A high axillary skin incision is made that is about 6cms long in the skin crease just lateral to the edge of the pectoral muscle. Once through the skin blunt dissection with a finger is carried into the submuscular place superiorly towards the clavicle. Once the clavicle is reached the finger is turned downward sweeping across the top of the ribs.
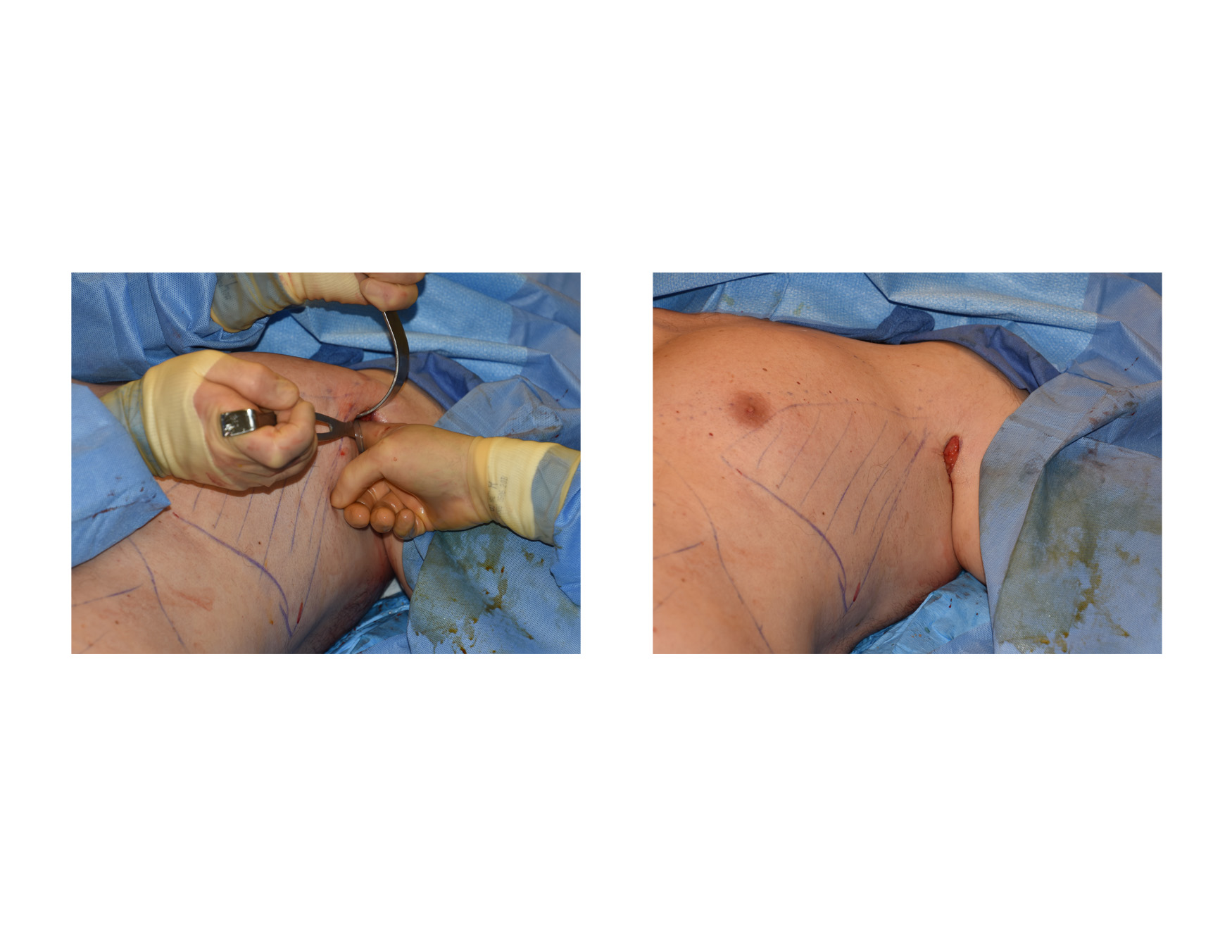
 A special instrument (Dingman-Agris dissector) is then inserted through the incision into the submuscular pocket created by the finger dissection. The instrument is used to make and reach the extent of the submuscular pocket. It is of critical importance that the lateral edge of the pectoral muscle attachments not be disrupted. (this is in contrast to that of making a breast implant pocket where the implant must go further to the side) The submuscular pocket is then washed out with saline until clear.
A special instrument (Dingman-Agris dissector) is then inserted through the incision into the submuscular pocket created by the finger dissection. The instrument is used to make and reach the extent of the submuscular pocket. It is of critical importance that the lateral edge of the pectoral muscle attachments not be disrupted. (this is in contrast to that of making a breast implant pocket where the implant must go further to the side) The submuscular pocket is then washed out with saline until clear.
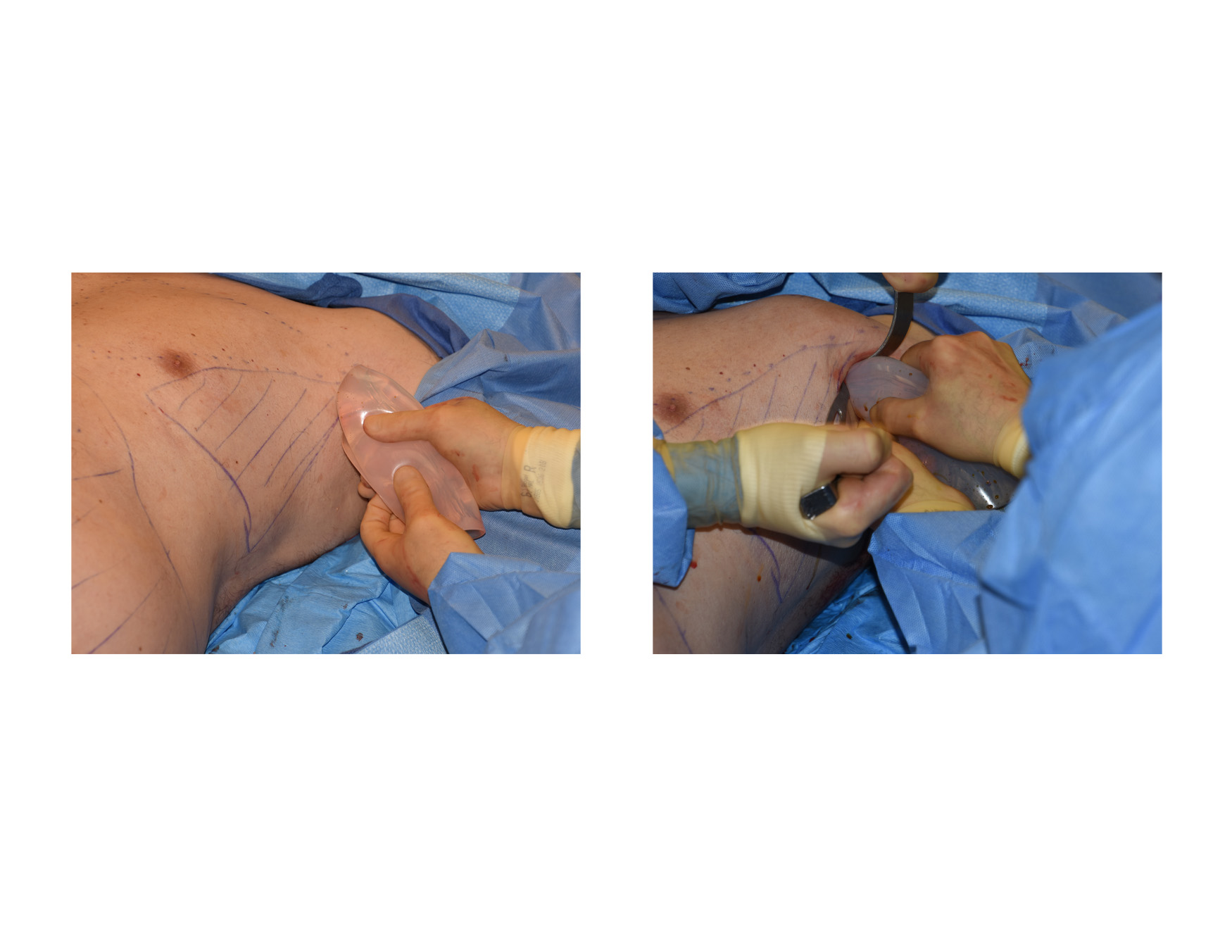
 The insertion of a pectoral implant requires that it be folded in half. In so doing and in the insertion process, it is important that the implant does not get torn or its shape disrupted. This is an important feature of how the implant is made. This is why I prefer using Implantech’s PowerFlex pectoral implants. They are made with a soft durometer but have a more stout silicone layer on their outside. This provides some ‘toughness ‘ to the implant so it can be inserted through much smaller incisions than its width would suggest it could. Once inserted the implant will unfold itself and can be slide into position.
The insertion of a pectoral implant requires that it be folded in half. In so doing and in the insertion process, it is important that the implant does not get torn or its shape disrupted. This is an important feature of how the implant is made. This is why I prefer using Implantech’s PowerFlex pectoral implants. They are made with a soft durometer but have a more stout silicone layer on their outside. This provides some ‘toughness ‘ to the implant so it can be inserted through much smaller incisions than its width would suggest it could. Once inserted the implant will unfold itself and can be slide into position.
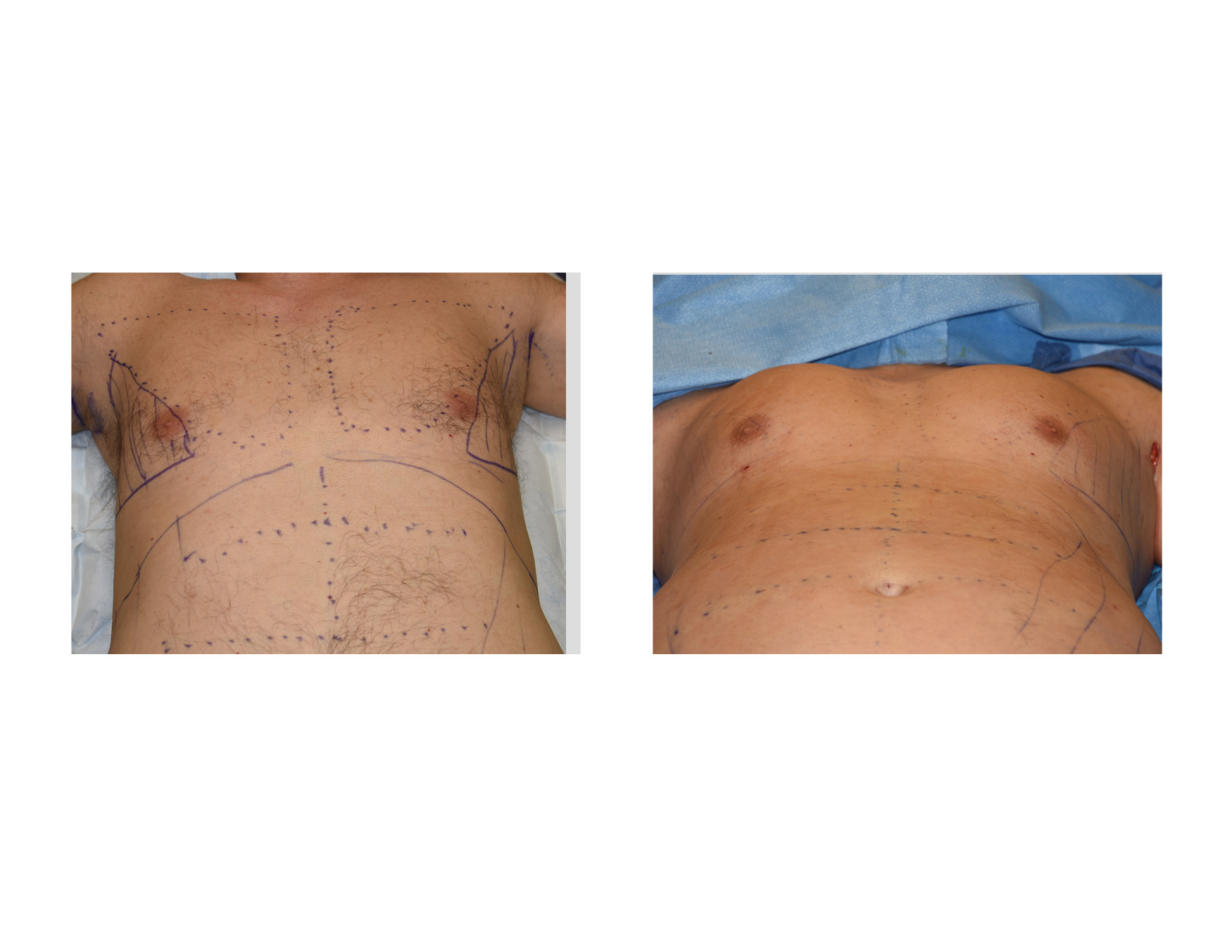 Once the incisions are closed, most men will benefit by liposuction of the lateral pectoral triangle that lies from the outer edge of the pectoralis major muscle onto the chest wall.This helps define the margins of the edge of the pectoralis muscle by contrasting the increased convexity of the muscle prominence with the increased concavity of the side of the chest.
Once the incisions are closed, most men will benefit by liposuction of the lateral pectoral triangle that lies from the outer edge of the pectoralis major muscle onto the chest wall.This helps define the margins of the edge of the pectoralis muscle by contrasting the increased convexity of the muscle prominence with the increased concavity of the side of the chest.
Dr. Barry Eppley
Indianapolis, Indiana