

Paranasal augmentation has been done using various techniques for differing anatomic reasons. By history paranasal augmentation meant the placement of a bony implant for a skeletally deficient midface often done in conjunction with rhinoplasty typically in Asian patient with flatter midface profiles. Since the introduction of injectable fillers and with increasing use of fat injections, paranasal augmentation has partially come to mean a soft tissue treatment of the deep nasolabial fold by the side of the nose. The most contemporary concept of paranasal augmentation is that it can be done for a variety of bony and soft tissue purposes but the implant is bone-based to do so.
 While differing paranasal implants have been available, they typically are of either preformed shapes or are done with layered ePTFE sheets. While each type of construct has its merits, I have to prefer to hand carve the paranasal implants out of an ePTFE block. This allows for a wide variety of adjustments for its size and thickness. Technically such hand carved midface implants are better called paranasal-maxillary implants as that more aptly describes their actual bony surface coverage. This creates a more natural type of augmentation and avoids the typical ‘bump’ feel and look from many traditional smaller paranasal implants.
While differing paranasal implants have been available, they typically are of either preformed shapes or are done with layered ePTFE sheets. While each type of construct has its merits, I have to prefer to hand carve the paranasal implants out of an ePTFE block. This allows for a wide variety of adjustments for its size and thickness. Technically such hand carved midface implants are better called paranasal-maxillary implants as that more aptly describes their actual bony surface coverage. This creates a more natural type of augmentation and avoids the typical ‘bump’ feel and look from many traditional smaller paranasal implants.
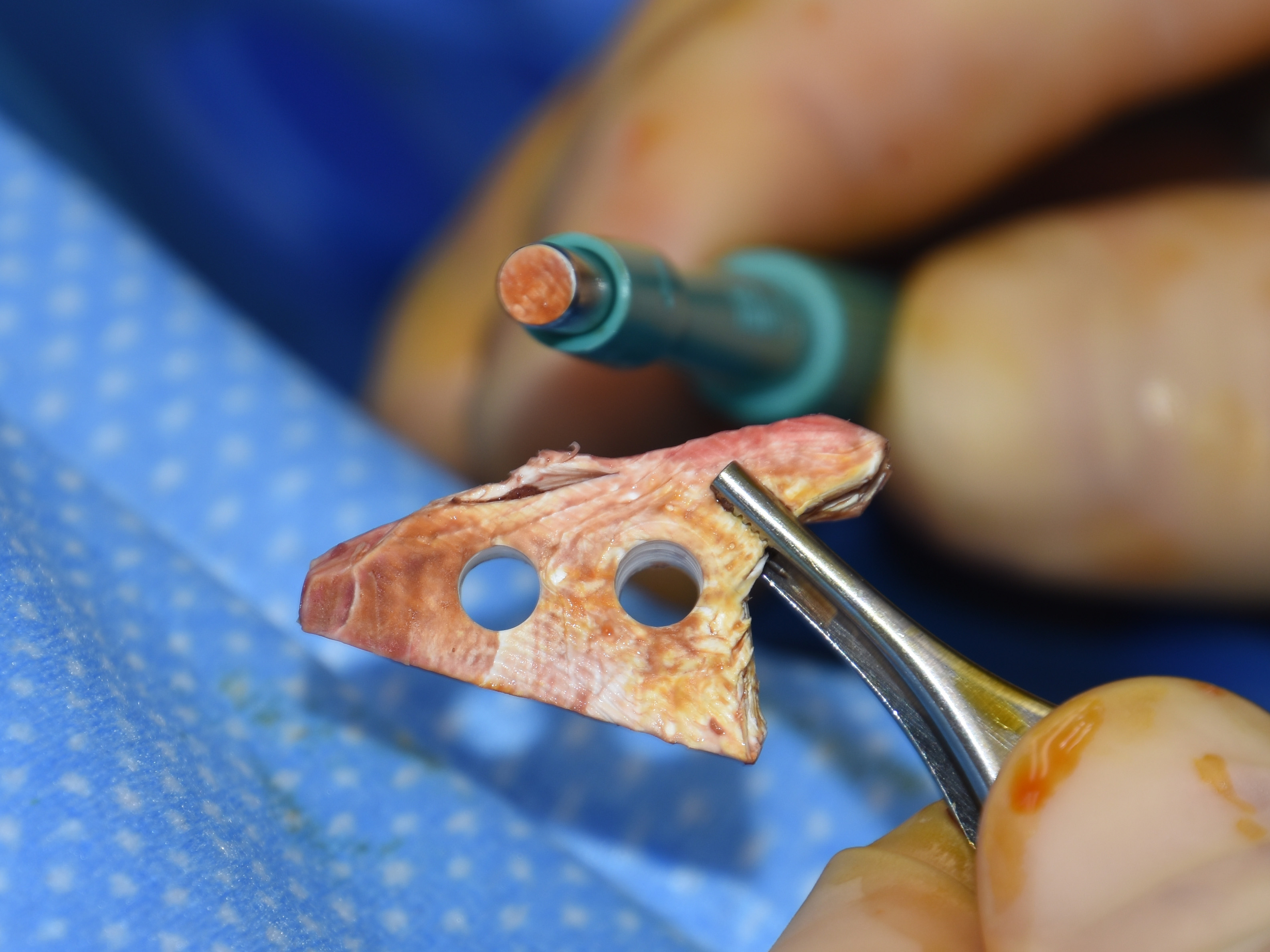
 While a hand carved ePTFE paranasal-maxillary implant can be secured by screw fixation, a more versatile technique is the placement of large perfusion holes through the implant. The tight subperiosteal pocket allows little room for any implant migration/movement and once tissue ingrowth occurs through the holes, which occurs quite quickly after surgery, firm fixation is permanently achieved.
While a hand carved ePTFE paranasal-maxillary implant can be secured by screw fixation, a more versatile technique is the placement of large perfusion holes through the implant. The tight subperiosteal pocket allows little room for any implant migration/movement and once tissue ingrowth occurs through the holes, which occurs quite quickly after surgery, firm fixation is permanently achieved.
The perforated ePTFE paranasal-maxillary implant provides good central midface augmentation, is made and adapted to each patient, and quickly achieve softvtissue integration both on its surface as well as through its perforations.
Dr. Barry Eppley
Indianapolis, Indiana