


The intricacies of the shape of the lower jaw can not be appreciated looking at plain x-rays like a panorex where it has been most commonly seen in its entirety. It is often perceived as largely being a smooth surface around its perimeter which it certainly is based on plain x-rays. And very many types of bone surgeries performed on it (e.g., sagittal split osteotomies or fracture repairs) such a perception is adequate to successfully perform the needed procedures. But between contemporary aesthetic jaw augmentation surgery and the now common availability of 3D CT scans a new level of anatomic appreciation has evolved.
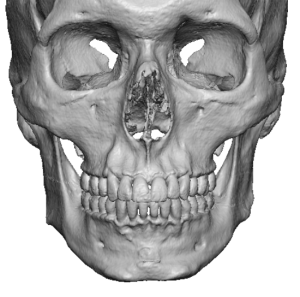
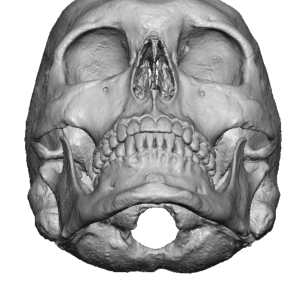 These new anatomic insights are most relevant in the jaw angle or mandibular ramus region. Rather than being a flat surface much of the ramus has an inner concavity surrounding by a more raised linear borders at its anterior, inferior and posterior areas. This concavity serves the purpose of where the bulk of the masseter muscle resides. While the end insertion of the masseter muscle is all along these outer linear borders these muscle attachments are predictably not nearly as thick as they are more centrally in the ramus. As a result to accommodate this large muscle mass the bone has a concavity where it sits and where the power is needed to generate jaw movement.
These new anatomic insights are most relevant in the jaw angle or mandibular ramus region. Rather than being a flat surface much of the ramus has an inner concavity surrounding by a more raised linear borders at its anterior, inferior and posterior areas. This concavity serves the purpose of where the bulk of the masseter muscle resides. While the end insertion of the masseter muscle is all along these outer linear borders these muscle attachments are predictably not nearly as thick as they are more centrally in the ramus. As a result to accommodate this large muscle mass the bone has a concavity where it sits and where the power is needed to generate jaw movement.

 There are gender differences in the depth of the muscle fossa of the ramus. To no surprise many men have deeper and more pronounced fossa depths due to a larger and thicker masseter muscle.
There are gender differences in the depth of the muscle fossa of the ramus. To no surprise many men have deeper and more pronounced fossa depths due to a larger and thicker masseter muscle.
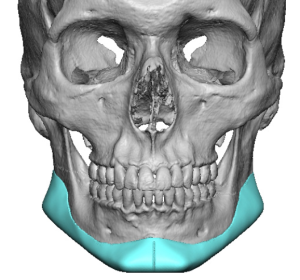 From an aesthetic standpoint augmentation of the jaw angles by implants must take this 3D ramus shape into consideration. Much of jaw angle implants are designed to make the lower edge of the muscular origin along the linear borders to have a more apparent shape. (some refer to this as squaring out the jaw angles but this is not an accurate geometric change that many patients need) The goal often is to make the skeletal border overcome the projection of the muscle mass above it. Which is why the shape of these implants become less thick as they ascend superiorly up the ramus.
From an aesthetic standpoint augmentation of the jaw angles by implants must take this 3D ramus shape into consideration. Much of jaw angle implants are designed to make the lower edge of the muscular origin along the linear borders to have a more apparent shape. (some refer to this as squaring out the jaw angles but this is not an accurate geometric change that many patients need) The goal often is to make the skeletal border overcome the projection of the muscle mass above it. Which is why the shape of these implants become less thick as they ascend superiorly up the ramus.
But there are patients who want a fuller muscular look to the jaw angles…meaning they want a more rounded look above the bottom of the jaw angles. You might call this a muscular jaw angle look. As there is no standard jaw angle implant that can create that effect it has to be done by custom design. If this was only a jaw angle implant a custom design could easily be created. But if it is desired as a component of a custom jawline implant it can be designed to do so but placement will be very difficult. The size of the implant that would create would require it to be segmentalize (sectioned into pieces) to get introduced into the pocket.

 An alternative approach for the custom jawline implant is to add to the initial implant design at the time of surgery an additional implant to create that muscular effect. One option to do so is to use a standard implant that is actually designed for a muscular augmentation effect. The style 1 temporal implant can be used to lay over the jawline implant to extend its augmentation more superiorly into the thicker part of the masseter muscle.
An alternative approach for the custom jawline implant is to add to the initial implant design at the time of surgery an additional implant to create that muscular effect. One option to do so is to use a standard implant that is actually designed for a muscular augmentation effect. The style 1 temporal implant can be used to lay over the jawline implant to extend its augmentation more superiorly into the thicker part of the masseter muscle.
 When using an overlay implant, even if it doesn’t cover all of the underlying implant, needs screw fixation beyond that used for the jawline implant. It is important to be aware that the temporal implants is much softer than all other facial implants so screw fixation must be applied ‘lightly’.
When using an overlay implant, even if it doesn’t cover all of the underlying implant, needs screw fixation beyond that used for the jawline implant. It is important to be aware that the temporal implants is much softer than all other facial implants so screw fixation must be applied ‘lightly’.
Dr. Barry Eppley
World-Renowned Plastic Surgeon