



 The long upper lip can only be treated by shortening the skin distance between the base of the nose and the vermilion-skin border. The subnasal lip lift is the most known and commonly performed of all the surgical lip enhancement procedures to achieve this effect. Its appeal is that it places the incision under the nose along the nasal base-lip crease for a relatively hidden scar.
The long upper lip can only be treated by shortening the skin distance between the base of the nose and the vermilion-skin border. The subnasal lip lift is the most known and commonly performed of all the surgical lip enhancement procedures to achieve this effect. Its appeal is that it places the incision under the nose along the nasal base-lip crease for a relatively hidden scar.
While this is certainly a favorable scar location what is overlooked is that the subnasal lip lift does not shorten or lift the entire upper lip. Its effect is most pronounced in the central cupid’s bow region which lies directly below where most of the skin excision occurs. There is a diminishing lifting effect along the vermilion border the more lateral one goes. By the time one get close to the mouth corner there is no effect at all. I have read surgeon’s comments numerous times that the subnasal lip lift can lift the lateral vermilion but this simply is not so…nor is it anatomically possible.
If one has good or fairly even vermilion upper lip fullness all the way out to the mouth corners, the subnasal lift will have an adequate full upper lip effect. Meaning that as the central vermilion is vertically moved upward the sides of the upper lip will still look proportionate. However if the sides of the vermilion of the upper lip fade into oblivion (turn in and disappear before the corner of the mouth) a subnasal lip lift will create an upper lip vermilion disproportion with the central lip vermilion looking too full compared to the sides. (also called the ‘rodent’ upper lip look)
One can and should test whether a good or adverse effect will be created with the subnasal lip lift by using the Q-tip test. By placing the wooden end of a Q-tip under the base of the nose and pushing inward a partial simulation of what the procedure will do may be seen. If the upper lip looks peculiar by doing so (central vermilion much fuller than the sides) then one needs to either not do the procedure….or considering combined it with lateral vermilion advancements.
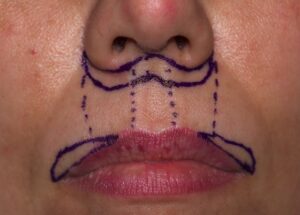
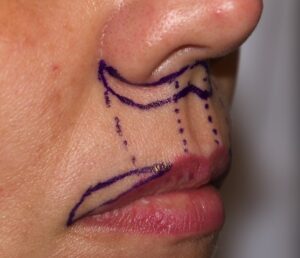 The lateral vermilion advancement elevates the position of the lateral vermilion from the mouth corner inward. As a general rule how far it extends towards the cupid’s bow is that it should fade completely away at a vertical line dropped down from the side of the nostrils…where the effect of the subnasal lip lift starts to dissipate. A key shape feature of the lateral vermilion advancement is that it is vertically greatest next to the mouth corner. If not the sides of the vermilion will still disappear before the vermilion ends at the mouth corner.
The lateral vermilion advancement elevates the position of the lateral vermilion from the mouth corner inward. As a general rule how far it extends towards the cupid’s bow is that it should fade completely away at a vertical line dropped down from the side of the nostrils…where the effect of the subnasal lip lift starts to dissipate. A key shape feature of the lateral vermilion advancement is that it is vertically greatest next to the mouth corner. If not the sides of the vermilion will still disappear before the vermilion ends at the mouth corner.

 Like the subnasal lip lift, and perhaps even more so, vermilion advancements must be very precisely excised and closed. There is little room for error in regards to placement at the vermilion-cutaneous border, symmetric excisional placement and fine line closure.
Like the subnasal lip lift, and perhaps even more so, vermilion advancements must be very precisely excised and closed. There is little room for error in regards to placement at the vermilion-cutaneous border, symmetric excisional placement and fine line closure.
Dr. Barry Eppley
Indianapolis, Indiana