

The treatment options for small shoulders or lack of adequate/desired deltoid muscle size has historically been the placement of implants. True deltoid implants as an off-the-shelf device does not exist due to lack of patient demand. But when a patient does request deltoid implants, they can be done using other modified body implants or they can be custom made.
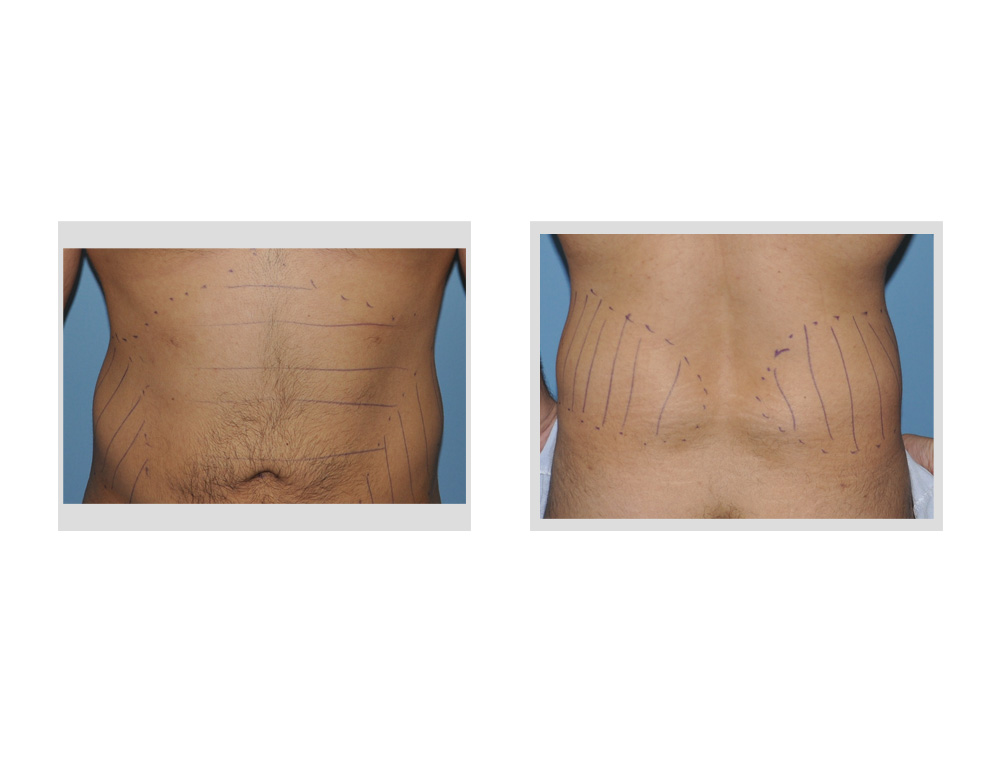 As an alternative option to implants for deltoid/shoulder augmentation, injectable fat can be used. Its use is predicated on whether the patient has enough fat to harvest to make the procedure worthwhile and the patient’s acceptance of wide variability of injected fat survival. Since men make up every deltoid augmentation patient I have ever seen, the fat donor sites are the traditional stomach and flanks (love handle) areas. Deltoid augmentation by fat injections provides a potentially pleasing dual benefit of abdominal and waistline reduction and an increase in shoulder size. (a body inversion if you will)
As an alternative option to implants for deltoid/shoulder augmentation, injectable fat can be used. Its use is predicated on whether the patient has enough fat to harvest to make the procedure worthwhile and the patient’s acceptance of wide variability of injected fat survival. Since men make up every deltoid augmentation patient I have ever seen, the fat donor sites are the traditional stomach and flanks (love handle) areas. Deltoid augmentation by fat injections provides a potentially pleasing dual benefit of abdominal and waistline reduction and an increase in shoulder size. (a body inversion if you will)
 When injecting fat into the deltoid shoulder area, I prefer to use a triangulation technique through three distinct entrance sites. The fat is injected both above the fascia in the subcutaneous fat as well as into the deltoid muscle below the fascia in small linear tracts of deposited fat. It usually takes about 100cc to 150cc per shoulder to produce an optimal amount of augmentation. For both shoulders this is a total amount of fat needed in the range of 250cc to 300cc. Since lipoaspirated fat must be concentrated prior to injection and such concentrations in men produce yields of 20% to 25% of the aspirate due to the higher fibrous content of their fat, it is necessary to ideally obtain at least 750cc to 1000cc of fat aspirate.
When injecting fat into the deltoid shoulder area, I prefer to use a triangulation technique through three distinct entrance sites. The fat is injected both above the fascia in the subcutaneous fat as well as into the deltoid muscle below the fascia in small linear tracts of deposited fat. It usually takes about 100cc to 150cc per shoulder to produce an optimal amount of augmentation. For both shoulders this is a total amount of fat needed in the range of 250cc to 300cc. Since lipoaspirated fat must be concentrated prior to injection and such concentrations in men produce yields of 20% to 25% of the aspirate due to the higher fibrous content of their fat, it is necessary to ideally obtain at least 750cc to 1000cc of fat aspirate.
 Since the shoulders are curved, injecting fat into them is best done with a similarly curved injection cannula. This allows the fat to be injected is the most even fashion possible whether above or below the deltoid fascia.
Since the shoulders are curved, injecting fat into them is best done with a similarly curved injection cannula. This allows the fat to be injected is the most even fashion possible whether above or below the deltoid fascia.
Deltoid augmentation with fat injections is a good alternative to implants that can be successful if one has enough donor fat. Optimal fat take requires a good concentration method and distribution of the fat by small linear track layering both above or below the deltoid muscle fascia
Dr. Barry Eppley
Indianapolis, Indiana