


Jaw angle augmentation with implants has become popular both as an isolated procedure as well as part of total jawline augmentation. In placing implants over the bony jaw angle region it is necessary to elevate the internal surface of the masseter muscle off of the bone. And in some cases when the implant needs to vertically lengthen the natural inferior border of the bone the musculoperiosteal layer must be elevated from the bottom side of the bone as an intact soft tissue sling. As an intact sling the implant can push the muscle down with it.
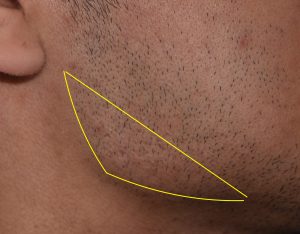 When the muscle fails to fully cover the implant or does not follow it downward with implant lengthening, a resultant soft tissue deficiency can occur over the angle of the implant. This is most commonly referred to as a masseter muscle dehiscence. But postoperative soft tissue defects over the augmented angle can also occur from an implant that has exceeded the ability of the muscle to completely cover it (implant reveal in which the muscle is not really torn) and when the width and flare of the implant creates a pseudo soft tissue deficiency above it.
When the muscle fails to fully cover the implant or does not follow it downward with implant lengthening, a resultant soft tissue deficiency can occur over the angle of the implant. This is most commonly referred to as a masseter muscle dehiscence. But postoperative soft tissue defects over the augmented angle can also occur from an implant that has exceeded the ability of the muscle to completely cover it (implant reveal in which the muscle is not really torn) and when the width and flare of the implant creates a pseudo soft tissue deficiency above it.
Almost regardless of the cause trying to get the muscle over the implant by repositioning is not usually effective. And it requires a neck incision to do so which has its own aesthetic liabilities…which are particularly apparent if the muscle repositioning does not work.
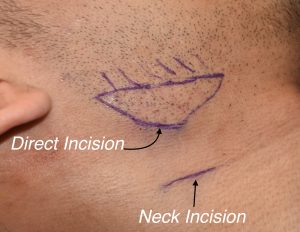 The alternative strategy to after implant jaw angle soft tissue deficiencies is a camouflage approach of which there are a variety of materials and grafts to do so. Injectable synthetic fillers and fat injections are the obvious methods of which lack of permanence (fillers) and lack of sustained volume (fat) are their disadvantages. Other options require an open approach for the placement allogeneic dermal grafts or subcutaneous soft tissue implants. In the placement of the latter, the incisional options include the traditional neck incision in a skin crease below the jaw angle or a smaller direct incision right behind the jaw angle prominence. In men this usually places it at the junction of the beard and non-hair bearing skin.
The alternative strategy to after implant jaw angle soft tissue deficiencies is a camouflage approach of which there are a variety of materials and grafts to do so. Injectable synthetic fillers and fat injections are the obvious methods of which lack of permanence (fillers) and lack of sustained volume (fat) are their disadvantages. Other options require an open approach for the placement allogeneic dermal grafts or subcutaneous soft tissue implants. In the placement of the latter, the incisional options include the traditional neck incision in a skin crease below the jaw angle or a smaller direct incision right behind the jaw angle prominence. In men this usually places it at the junction of the beard and non-hair bearing skin.

 The posterior jaw angle incision can be shorter than the neck incision because it provides direct access. This allows the muscle position to be assessed and manipulated if desired but, more relevantly, allows the placement of a tissue bank dermal graft over the soft tissue deficiency area right under the skin where it has the biggest impact. Such dermal grafts need to be at least 2mms thick to have an adequate contouring effect.
The posterior jaw angle incision can be shorter than the neck incision because it provides direct access. This allows the muscle position to be assessed and manipulated if desired but, more relevantly, allows the placement of a tissue bank dermal graft over the soft tissue deficiency area right under the skin where it has the biggest impact. Such dermal grafts need to be at least 2mms thick to have an adequate contouring effect.
 The direct incision is both a safe approach as it lies above the frontal branch of the facial nerve and heals better than a neck incision. Such jaw angle soft tissue augmentations can be comfortably done under local anesthesia with minimal recovery.
The direct incision is both a safe approach as it lies above the frontal branch of the facial nerve and heals better than a neck incision. Such jaw angle soft tissue augmentations can be comfortably done under local anesthesia with minimal recovery.
An interesting observation I have made through the direct incision is that most of the time muscle fibers are present over the implant. This challenges the perception in some patients as to whether masseteric muscle retraction is the correct diagnosis. Perhaps it is just partial muscle retraction of the inner fibers but not the whole thickness of the muscle.
Dr. Barry Eppley
Indianapolis, Indiana