

Shoulder reduction by removing a segment of the clavicle bone is an effective procedure for decreasing the bideltoid width. A 2.5 to 3cm segment of bone is removed from the inner third of each clavicle which is both the location of the thickest diameter of the bone as well as the most favorable location for the small incision needed to do it. (supraclavicular fossa) The bone segments are brought together to achieve the reduction and stabilized with a superior fixation plate and screws.
While an effective procedure it does pose some unique challenges for the patient’s recovery. Because it is a bilateral procedure (done on both shoulders) there are significant arm movement restrictions that are in place for the first month after surgery. While patients deal with these restrictions well and gone on to a full recovery, it is nonetheless challenging for them. For this reason I have heard of some surgeons performed the procedure only on one shoulder at a time. While this would certainly make each recovery less challenging it still means there will be two separate surgeries and recoveries. In my experience the single superior plate fixation in clavicle reduction osteotomies works well. I never had a problem in dozens of shoulder width reduction surgeries until last year when one patient developed fixation failure on one side several weeks after the procedure. While that satisfactorily revolved by a revisional surgery with application of double plates, it raised the question of whether every patient should have such double plates for maximal assurance of uncomplicated healing. The use of double plate fixation should also allow the patient the potential for earlier range of arm motion.

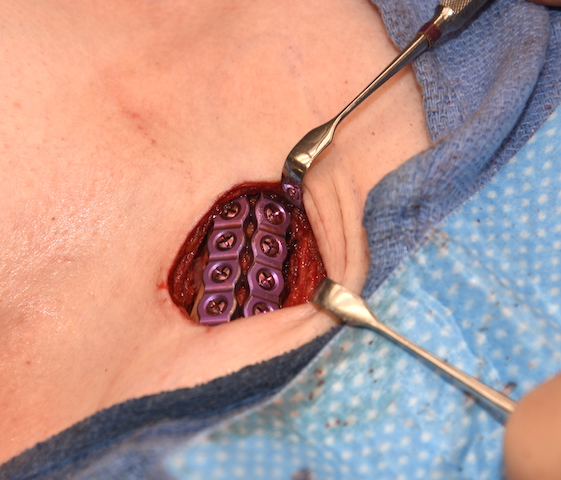
 In double plate fixation of clavicle reduction osteotomies the first fixation device applied is a 2.7mm plate applied to the superior aspect of the bone with 3 screws per side. The second plate is applied to the anterior surface of the bone which is also a 2.7mm plate with two screws on each side of the osteotomy.
In double plate fixation of clavicle reduction osteotomies the first fixation device applied is a 2.7mm plate applied to the superior aspect of the bone with 3 screws per side. The second plate is applied to the anterior surface of the bone which is also a 2.7mm plate with two screws on each side of the osteotomy.
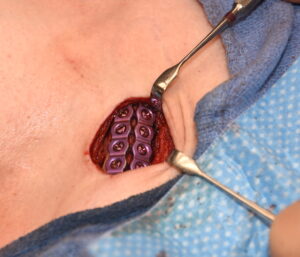 A single superior plate on the clavicle resists bone displacement with lateral arm elevation but is less effective at resisting front to back rotational forces. The anterior plate resists such rotational displaying forces. Given that it is two round bone edges directly against each other the use of double plates should allow for rapid bone healing. Earlier arm motion may then be permitted.
A single superior plate on the clavicle resists bone displacement with lateral arm elevation but is less effective at resisting front to back rotational forces. The anterior plate resists such rotational displaying forces. Given that it is two round bone edges directly against each other the use of double plates should allow for rapid bone healing. Earlier arm motion may then be permitted.
While the use of double plate fixation adds additional costs to shoulder width reduction surgery, avoiding the risk of fixation failure and a second surgery to fix it is well worth it. Add in the capability of earlier range of motion during the recovery period adds to its value.
Dr. Barry Eppley
Indianapolis, Indiana