


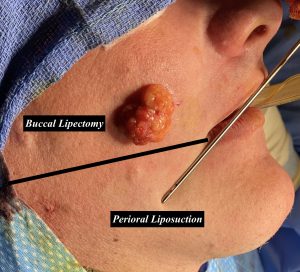
Making the cheeks less full or slimmer typically refers to reduction of the soft tissue trampoline area of the midface. Sandwiched between the cheekbones and the bony jawline are the soft tissues of the cheek which are suspended like a trampoline between these bony attachments. The only tissue removal that can be done in the trampoline area is fat and the buccal lipectomy is the most recognized soft tissue cheek reduction procedure. While effective given its discrete encapsulated fat collection it does not affect the entire trampoline area. Its reductive effects are limited to the upper half of the trampoline area. Only in cases of buccal fat pad prolapse, which is rare, is any fullness in the lower half of the trampoline area due to this unique facial fat pad.
The fat in the lower half of the trampoline area is largely subcutaneous in location like many other areas in the body. Its removal requires liposuction which is why this specific area of facial fat removal is known as perioral liposuction. Done from a nick incision inside the mouth corner very small cannulas are used to aspirate this fat area. Because of the access point this is why it is called perioral but the extent of the treated area is only limited by the length of the cannula.
 Putting the two fat removal procedures of the cheek together creates a more complete reduction of the cheek trampoline area which for many patients is adequate. But in the difficult case of the full thick tissued cheek patient there is one additional cheek soft tissue reduction procedure which is excisional in nature. Done from an intraoral approach a horizontal wedge of mucosa, fat and buccinator muscle is done and then closed primarily. (buccinator myectomy) The three procedures done collectively truly maximize whatever amount of cheek reduction/concavity that can be created.
Putting the two fat removal procedures of the cheek together creates a more complete reduction of the cheek trampoline area which for many patients is adequate. But in the difficult case of the full thick tissued cheek patient there is one additional cheek soft tissue reduction procedure which is excisional in nature. Done from an intraoral approach a horizontal wedge of mucosa, fat and buccinator muscle is done and then closed primarily. (buccinator myectomy) The three procedures done collectively truly maximize whatever amount of cheek reduction/concavity that can be created.

 Because the combined perioral liposuction and buccinator myectomy creates a full thickness cheek injury postoperative compression would be beneficial to help with swelling and bruising reduction. But there is no cheek garment that can be effective. A very good method of compression is an external bolster in which through and through resorbable sutures are passed and tied down. This squeezes/compresses the two sides of the cheeks together. Maintained in placed for 1 to 2 days after the surgery is the usual time period for which it is maintained in place.
Because the combined perioral liposuction and buccinator myectomy creates a full thickness cheek injury postoperative compression would be beneficial to help with swelling and bruising reduction. But there is no cheek garment that can be effective. A very good method of compression is an external bolster in which through and through resorbable sutures are passed and tied down. This squeezes/compresses the two sides of the cheeks together. Maintained in placed for 1 to 2 days after the surgery is the usual time period for which it is maintained in place.

 While the compression that such an external bolster applies can be significant it is always possible to have too much compression…which could cause skin necrosis. Tying down the sutures therefore must be done with that risk in mind.
While the compression that such an external bolster applies can be significant it is always possible to have too much compression…which could cause skin necrosis. Tying down the sutures therefore must be done with that risk in mind.
Dr. Barry Eppley
World-Renowned Plastic Surgeon