

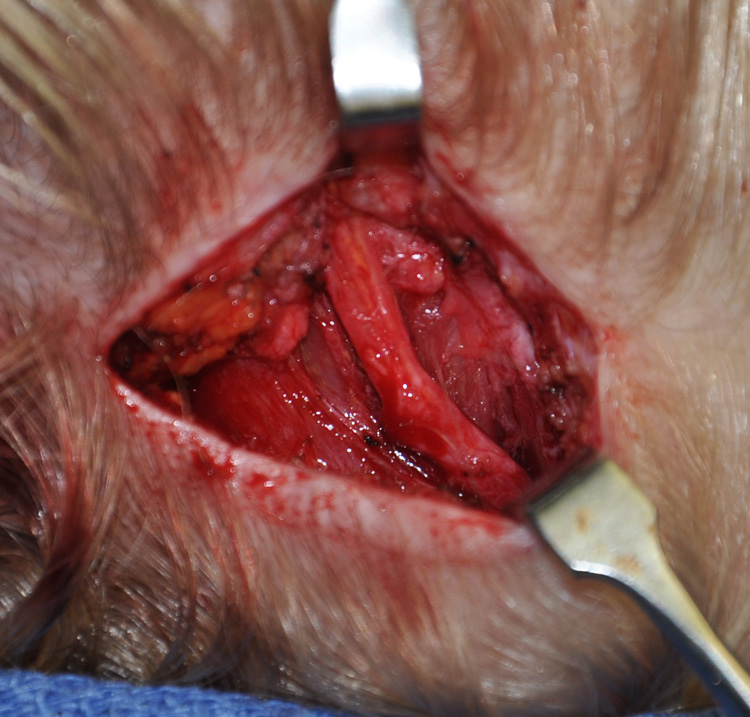
Contemporary migraine surgery for the treatment of perpheral triggers involves decompression of the involved nerves. The most common involved nerves include the supraorbital, supratrochlear and the greater and lesser occipital nerves. (the zygomaticotemporal and auriculotemporal nerves are avulsed so they are excluded) The success of nerve decompression depends on adequate release of the enveloping muscle and fascia so any pinching effect on the nerve is eliminated.
But decompressive migraine surgery does not always produce sustained relief and one of the reasons is recurrent compression due to scar formation. Despite being relieved of constructive muscle fibers, the surrounding tissues do have to heal and the space left behind can be replaced with scar tissue. Such scar tissue formation naturally contracts as it heals, thus potentially replicating the initial nerve compression problem.
 One simple strategy to prevent recurrent nerve compression in migraine surgery is the use of fat grafts. Placing a fat graft over or around the released nerve can have several beneficial effects. Its obvious benefit is that it fills the open space around the nerve from the release and provides a quickly revascularized soft tissue buffer from the surrounding tissues. The other potential benefit is less obvious and unproven but theoretically possible.
One simple strategy to prevent recurrent nerve compression in migraine surgery is the use of fat grafts. Placing a fat graft over or around the released nerve can have several beneficial effects. Its obvious benefit is that it fills the open space around the nerve from the release and provides a quickly revascularized soft tissue buffer from the surrounding tissues. The other potential benefit is less obvious and unproven but theoretically possible.
Fat tissue is seen today as an active and secreting organ that produces a variety of special proteins. One of these are neurotrophic factors such as nerve growth factor and brain-derived neurotrophic factor. Such factors are known to have a role in stimulating repair of peripheral nerves as well as a regulator of immune and inflammatory responses. Placing a fat graft against a nerve that has been compressed and inflamed may have a healing and reparative effect.
The harvest of a small fat graft is quick and easy and its placement onto the released nerve is similarly so. There is no morbidity in doing so and fat graft placement around the nerve can be done either in an open wound or in an endoscopic approach.
Dr. Barry Eppley
Indianapolis, Indiana