


The premaxilla is anatomically the piece of bone at the very end of the upper jaw. It contains the anterior incisor teeth which is why it is also called the incisive bone. It is embryologically distinct from the maxilla and is separated from it by a suture early in life. Aesthetically the projection of the premaxillary bone and incisor teeth as well as the anterior nasal spine above it have a major influence on the appearance of the base of the nose and the upper lip.
A premaxillary deficiency can be part of an overall midfacial growth destruction or rarely can exist in isolation. It is the most noticeable part of any midface deficiency because of its effect on the nasal base and the upper lip below it. It results in a flat or recessed appearance to the base of the columella and the nostrils. The nasolabial angle is more closed or acute. The skin of the upper lip can appear retruded. The nasolabial folds can appear prematurely deep.

 The definitive permanent option for augmenting the premaxilla or the central lower midface is a premaxillary implant. A limited number of implant options have been historically available for this part of the face. A more recent addition has been the ePTFE premaxillary implant. Composed of an expanded polytetraethylene material that develops soft issue adherence, it has a natural shape to the base of the nose that easily adapts to the anatomy without implant modification.
The definitive permanent option for augmenting the premaxilla or the central lower midface is a premaxillary implant. A limited number of implant options have been historically available for this part of the face. A more recent addition has been the ePTFE premaxillary implant. Composed of an expanded polytetraethylene material that develops soft issue adherence, it has a natural shape to the base of the nose that easily adapts to the anatomy without implant modification.
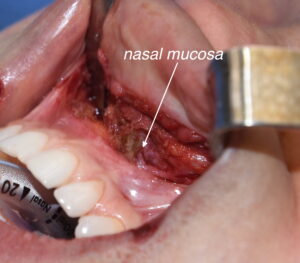 Premaxillary implants can be placed either through an intranasal or intraoral approach, both of which work successfully. In the intraoral approach a high vestibular incision is made between the canines. Leaving a good cuff of muscle and mucosa inferiorly, subperiosteal dissection is done around the pyriform aperture and across the bony anterior nasal spine. Care must be taken to not violate the nasal mucosa when doing so. And to have a good snug fit around the base of the nose the nasal mucosa must be well visualized.
Premaxillary implants can be placed either through an intranasal or intraoral approach, both of which work successfully. In the intraoral approach a high vestibular incision is made between the canines. Leaving a good cuff of muscle and mucosa inferiorly, subperiosteal dissection is done around the pyriform aperture and across the bony anterior nasal spine. Care must be taken to not violate the nasal mucosa when doing so. And to have a good snug fit around the base of the nose the nasal mucosa must be well visualized.

 The premaxillary implant can then be placed into the created pocket and secured with a midline suture to the septal cartilage over the anterior nasal spine. The material’s adaptability and tissue ingrowth obviate the need for screw fixation in most cases. In closing it it critically important to have a two-layer closure with an internal muscle layer over the implant and mucosa over the muscle.
The premaxillary implant can then be placed into the created pocket and secured with a midline suture to the septal cartilage over the anterior nasal spine. The material’s adaptability and tissue ingrowth obviate the need for screw fixation in most cases. In closing it it critically important to have a two-layer closure with an internal muscle layer over the implant and mucosa over the muscle.
Preformed ePTFE premaxillary implants are a good addition to mid facial implants with a favorable tissue characteristics and ease of secure surgical placement.
Dr. Barry Eppley
Indianapolis, Indiana