

In Type 1 rib removal surgery the primary goal is reduction in the length of the free floating ribs (#11 and #12) and any associated soft tissue thicknesses around them. The soft tissue removal can be two fold, flank fat by liposuction and latissimus dorsi (LD) muscle by excision. While rib removal surgery understandably has an emphasis on the bone component the significance of the muscle removal in particular is under appreciated.
The LD muscle is the largest muscle in the upper body and covers a significant portion of the lower thorax. What it is evident in anatomic renderings that the LD muscle extends out further on the waistline than the free floating ribs this become very evident when doing the actual surgery. As the first major structure that must be bypassed is the LD muscle to even get to the ribs. Thus it has always been logical that some reduction in its width would-be helpful in the goal of the rib removal surgery… a more narrow waistline.
In my early experience in rib removal surgery and how I did it for many years is a wedge reduction technique. The LD muscle was split transversely from its outer border inward enough to visualize the ribs. Then once rib removal is completed triangles of muscle above and below the horizontal split line were removed. While effective this occasionally left a sharper indentation at the waistline particularly fun thinner patients.

 Borrowing a technique used in more wide open rib removal surgeries (Type II – IV), the ribs are exposed by a longitudinal split in the LD muscle away from its lateral border. Once the ribs are removed their empty spaces are packed with Exparel-soaked Gelfoam sponges.
Borrowing a technique used in more wide open rib removal surgeries (Type II – IV), the ribs are exposed by a longitudinal split in the LD muscle away from its lateral border. Once the ribs are removed their empty spaces are packed with Exparel-soaked Gelfoam sponges.

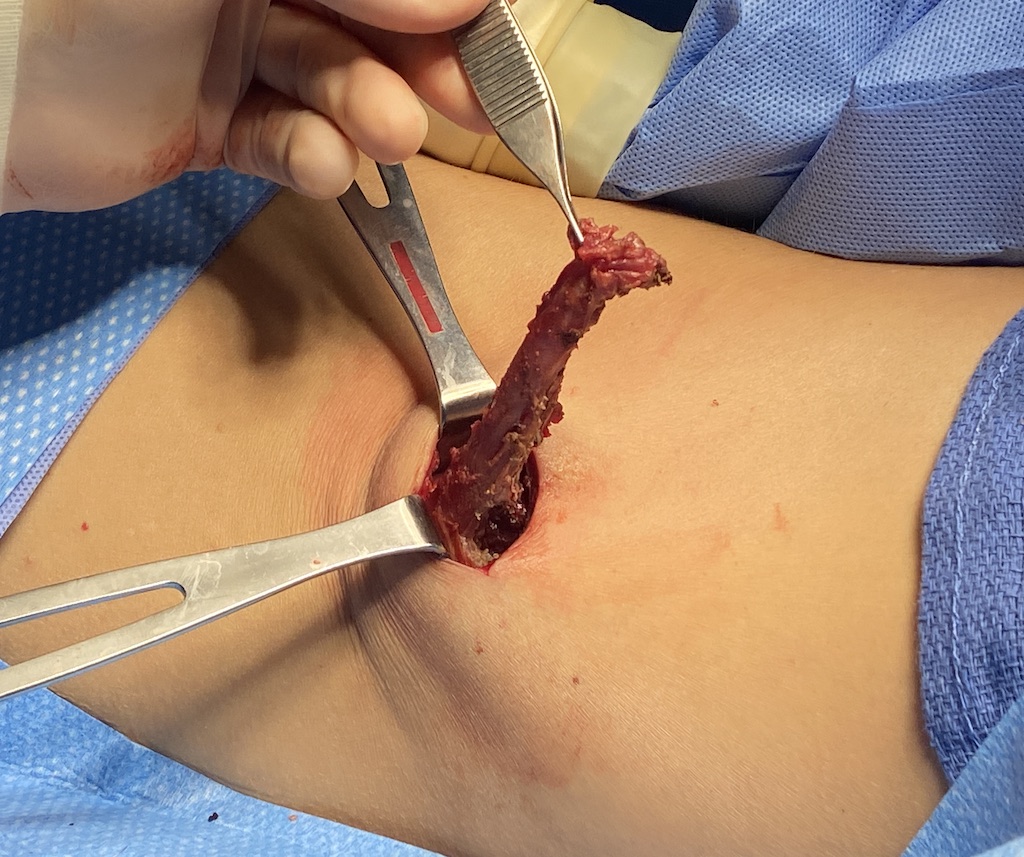
 Then a longitudinal excision of 2 to 3 cms of LD muscle width is removed, leaving the lateral border intact, as far inferior and superior than the incision will allow.
Then a longitudinal excision of 2 to 3 cms of LD muscle width is removed, leaving the lateral border intact, as far inferior and superior than the incision will allow.

 The longitudinal excision of the muscle is closed by a running suture, pulling in the lateral border of the muscle. This leaves a smooth lateral muscle border but still with an effective muscle width reduction in the target area. The incision is then closed over a drain.
The longitudinal excision of the muscle is closed by a running suture, pulling in the lateral border of the muscle. This leaves a smooth lateral muscle border but still with an effective muscle width reduction in the target area. The incision is then closed over a drain.
The LD muscle does add some width to the waistline due to its shape and location of its lateral border. Thus some reduction in its transverse width at the periumbilical line adds to the effects of free floating rib removal surgery. Not matter how the muscle reduction is done it has no negative effects on the function of the muscle. The longitudinal excision technique offers both exposure for rib removals as well as the maximal amount of muscle removal through such a small incision. It also ensures that a smooth lateral muscle border is maintained.
Dr. Barry Eppley
World-Renowned Plastic Surgeon