

Medpor implant material is well know to create vigorous soft tissue attachments due to its irregular surface contour. Such soft tissue adherence has both advantages and disadvantages. A major disadvantage is if the implant needs to be adjusted and/or removed. Getting the Medpor implant out has been stated by some to be impossible and most would consider it difficult at the least. Such removals are magnified by the tendency for surgeons to almost universally use screw fixation of the implant to the bone, often with a considerable number of screws used.
Since the chin is the most common location of aesthetic facial implant augmentations, Medpor chin implants and their requested removal is not uncommon. Whether this is done from intraoral or submental incisional approach does not change the surgical technique to do so.

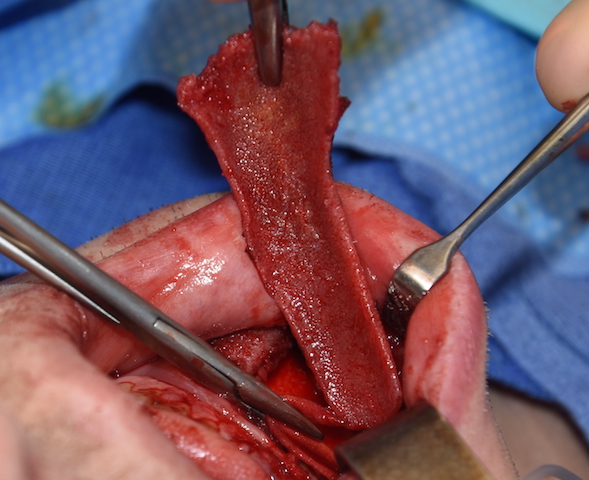
 When exposing a Medpor chin implant the midline split in the implant is first located. This exists in all such implants because their rigidity requires a two-piece insertion method. While a tab exist across the split from one side of the implant, the split is separated sharply with a scalpel down to the bone. This will then allow they implant to be lifted off of the bone. Should any screws exist (and there almost always is) I usually don’t try to remove them by unscrewing them. Rather the implant is lifted off and separated from the intact screw from below. Then the fully exposed threads of the screw allows it to be twisted off and removed.
When exposing a Medpor chin implant the midline split in the implant is first located. This exists in all such implants because their rigidity requires a two-piece insertion method. While a tab exist across the split from one side of the implant, the split is separated sharply with a scalpel down to the bone. This will then allow they implant to be lifted off of the bone. Should any screws exist (and there almost always is) I usually don’t try to remove them by unscrewing them. Rather the implant is lifted off and separated from the intact screw from below. Then the fully exposed threads of the screw allows it to be twisted off and removed.
 The Medpor implant can be lifted off the bone from underneath because there is no bony ingrowth into the material (which I have never seen) and the thick capsule which develops between the implant and the bone. (as occurs with any implant material) The implant is lifted off of the bone throughout its entire length which is safe to do so without injury to the mental nerve. Once the implant is off the bone then electrocautery is used on its outer surface to separate it from the overlying soft tissues. This is where the most adherent tissue attachments are. As one works further back the implant is continuously pulled forward to gain increasing posterior access. Attention must be particularly paid to two areas, the location of the mental nerve along the implant’s superior edge and to ensure that the very end of the implant is removed and not left behind. (which tends to easily break off)
The Medpor implant can be lifted off the bone from underneath because there is no bony ingrowth into the material (which I have never seen) and the thick capsule which develops between the implant and the bone. (as occurs with any implant material) The implant is lifted off of the bone throughout its entire length which is safe to do so without injury to the mental nerve. Once the implant is off the bone then electrocautery is used on its outer surface to separate it from the overlying soft tissues. This is where the most adherent tissue attachments are. As one works further back the implant is continuously pulled forward to gain increasing posterior access. Attention must be particularly paid to two areas, the location of the mental nerve along the implant’s superior edge and to ensure that the very end of the implant is removed and not left behind. (which tends to easily break off)

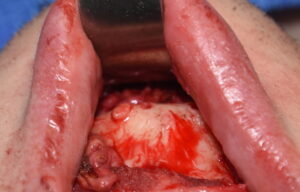
 Once one half of the chin implant is removed then the other half may be done similarly. Such Medpor chin implants can be removed both safely and in their entirety.
Once one half of the chin implant is removed then the other half may be done similarly. Such Medpor chin implants can be removed both safely and in their entirety.
 When removing Medpor implant materials the tissue reactions to them can be appreciated and are consistent. My observations are as follows:
When removing Medpor implant materials the tissue reactions to them can be appreciated and are consistent. My observations are as follows:
- The most adherent tissue attachments are on its external surface from the overlying soft tissues.
- Bone ingrowth does not occur into the material on its undersurface,
- Bony overgrowth along the sides is not seen.
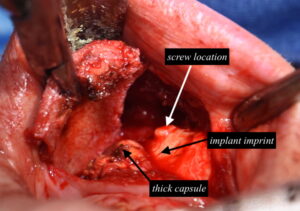
- A thick capsule develops between the implant and the bone.
- Implant imprinting on the bone occurs creating an outline on the bone.
- Bone imprinting of the implant does not occur around the base of the screws.
Dr Barry Eppley
Indianapolis, Indiana