

Smiling is the single most important facial expression. It takes a lot of facial muscles to smile and their pull causes surrounding facial structures to move beyond that of just the lips. The superiorly positioned nose can move when one smiles as the upper lip elevates. The flexible tip of the nose is what can change at either the tip or the nostrils.
 While nasal movement with smiling is usually regarded as incidental and not aesthetically bothersome, there are certain nasal movements that can be. The most common is the downturning of the nasal tip caused by a hyperactive depressor septi muscle. The more rare adverse aesthetic movement is an undesired elevation of the base of the nostrils. This is an upward and inward movement of the nostrils where they attach to the face. This is caused mainly by the quadratus labii superioris muscle.
While nasal movement with smiling is usually regarded as incidental and not aesthetically bothersome, there are certain nasal movements that can be. The most common is the downturning of the nasal tip caused by a hyperactive depressor septi muscle. The more rare adverse aesthetic movement is an undesired elevation of the base of the nostrils. This is an upward and inward movement of the nostrils where they attach to the face. This is caused mainly by the quadratus labii superioris muscle.
This muscle has two portions, the medial and lateral heads. The medial head is known as the levator labii superioris alaeque nasi muscle. This slip of the muscle originates from the frontal process of the maxilla and comes downward to insert into the alar cartilage and the skin of the nostril attachment to the face. (another slip of the muscle goes on to insert into the upper lip. Since muscles pull towards their origins it is this action that pulls the base of the nose upward.
Counteracting the action of the legator labii superiors alaeque nasi muscle can be done by disinsertion of the muscle from the nose. But to be absolutely certain that the action of the muscle is countered an addition technical maneuver can be helpful. Securing the base of the nose in a downward direction to the bone provides a point of fixation that can resist any residual muscle action.
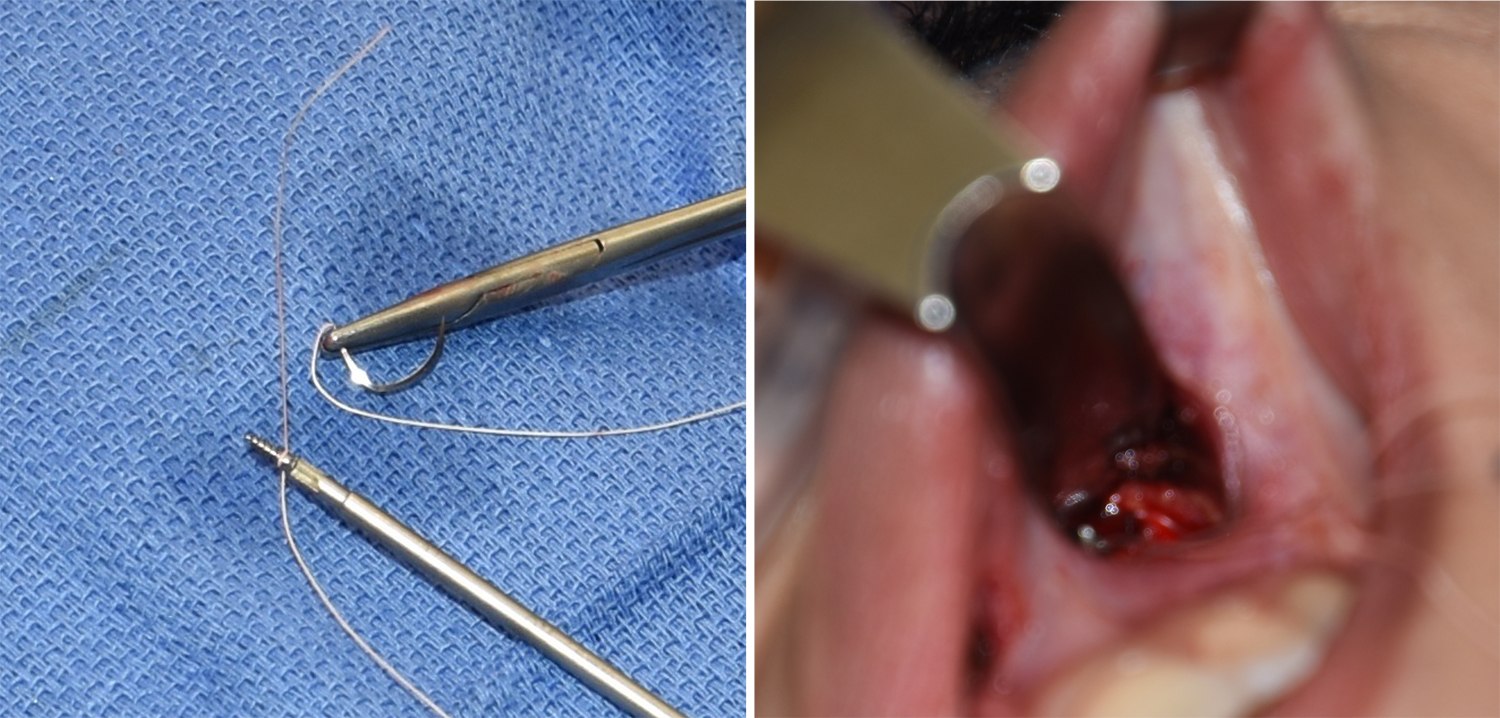
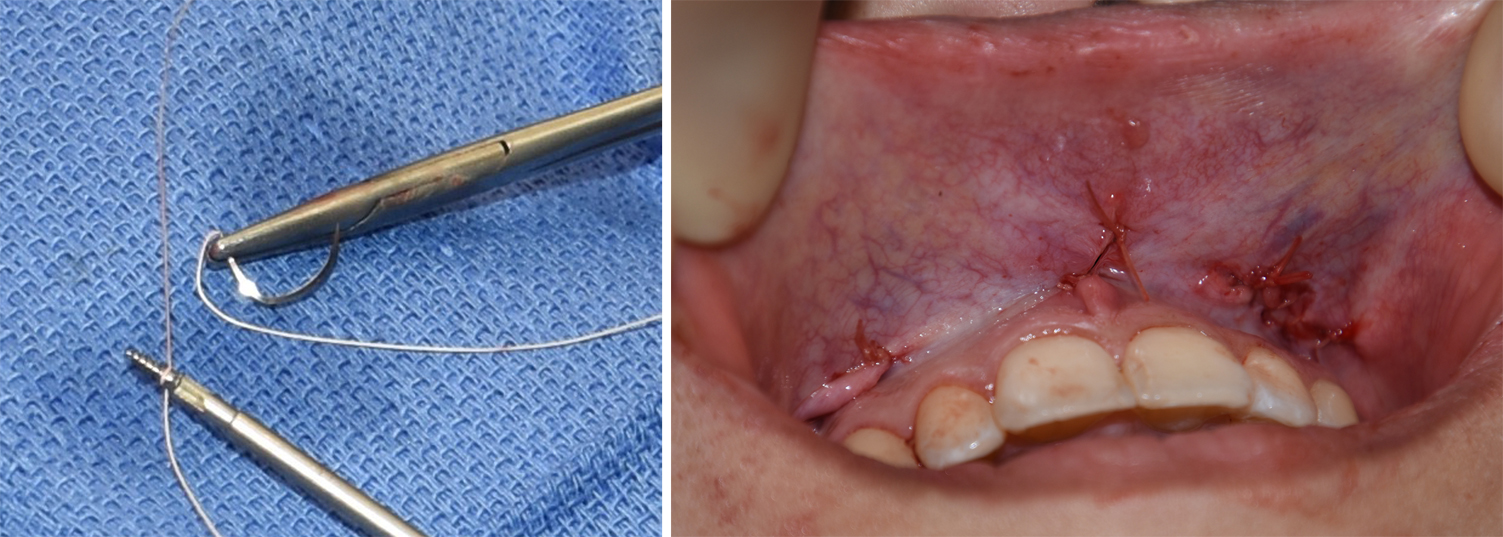 This is done by a bone anchoring technique to the pyriform aperture. Using a permanent 4-0 Tevdek suture attached to a 1.5mm x 5mm titanium microscrew, the anchor is initially placed into the bone through a small intraoral incision. The needle of the suture then takes a bite of tissue just under the nostril attachment. The suture is tied down loosely, making it tight but not cinching it down enough that it pulls the nostril inward.
This is done by a bone anchoring technique to the pyriform aperture. Using a permanent 4-0 Tevdek suture attached to a 1.5mm x 5mm titanium microscrew, the anchor is initially placed into the bone through a small intraoral incision. The needle of the suture then takes a bite of tissue just under the nostril attachment. The suture is tied down loosely, making it tight but not cinching it down enough that it pulls the nostril inward.
This intraoral bone anchoring technique provides firm fixation to prevent the nasal base from pulling upward when smiling. It is a useful adjunct to muscle release and provides a two-way approach to the nasal animation problem.
Dr. Barry Eppley
Indianapolis, Indiana