

As an aesthetic procedure mouth widening borrows some basic principles from reconstructive plastic surgery. Opening or expanding any aperture requires that its circumferential perimeter length be increased. In mouth widening there are two specific aperture areas to be increased that are directly across from each other. (sides of the mouth) This poses some stability concerns with the expansion which are helped somewhat by the mouth’s oblong shape.

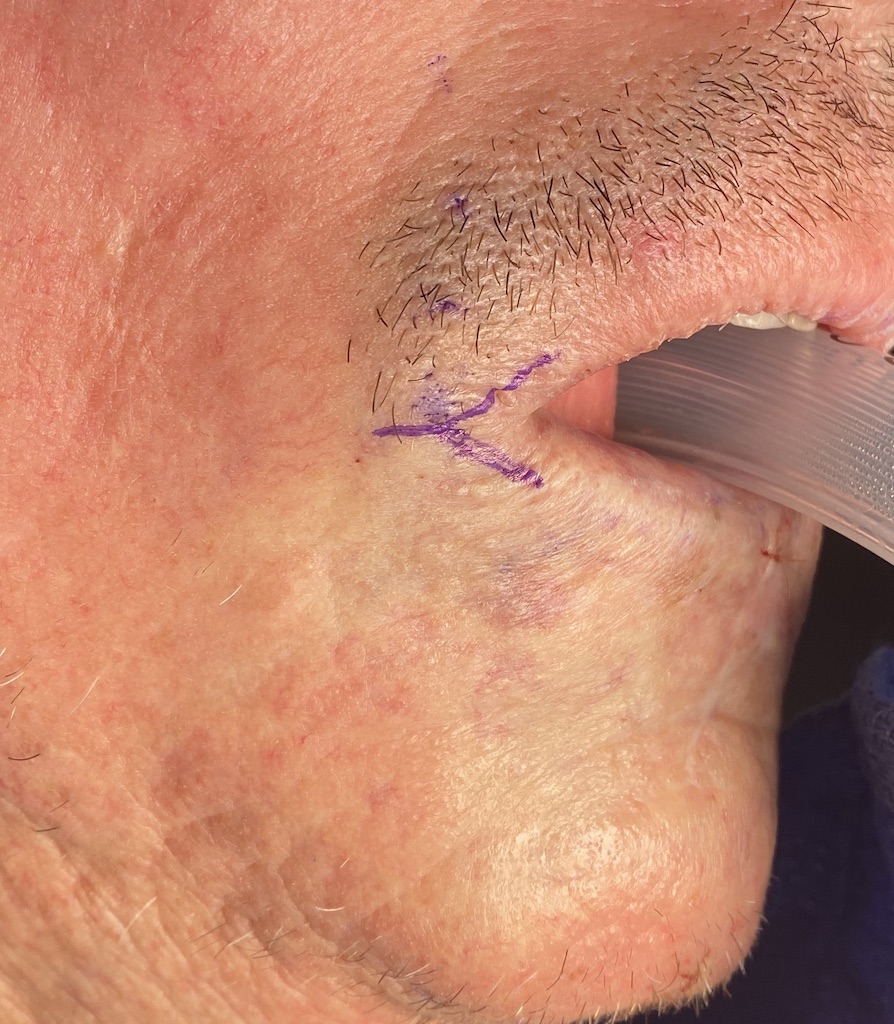
 Widening of the mouth corners is best conceptualized as lengthening a line or scar. In this case the line happens to be bent in the shape of an arrow. Making the mouth wider is taking this arrow shape and moving it out laterally…which is a Y-V advancement. This is the reverse of the well known V-Y scar lengthening technique. It works because it moves the mucosa of the mouth corner outward to fill the defect left by opening up a linear line of skin.
Widening of the mouth corners is best conceptualized as lengthening a line or scar. In this case the line happens to be bent in the shape of an arrow. Making the mouth wider is taking this arrow shape and moving it out laterally…which is a Y-V advancement. This is the reverse of the well known V-Y scar lengthening technique. It works because it moves the mucosa of the mouth corner outward to fill the defect left by opening up a linear line of skin.

 But with the opening of the linear line of skin the orbicularis muscle will be exposed. This circumferential ring of muscle around the mouth serves as an obstruction when trying to widen the mouth. Removing a wedge of the mouth is essential to allow an unobstructed placement of the new mouth corner. Muscle removal also serves to help prevent postoperative relapse as the muscle constricts on the new position of the mouth corners. This small wedge of muscle removal has no negative impact on postoperative mouth movements.
But with the opening of the linear line of skin the orbicularis muscle will be exposed. This circumferential ring of muscle around the mouth serves as an obstruction when trying to widen the mouth. Removing a wedge of the mouth is essential to allow an unobstructed placement of the new mouth corner. Muscle removal also serves to help prevent postoperative relapse as the muscle constricts on the new position of the mouth corners. This small wedge of muscle removal has no negative impact on postoperative mouth movements.
 Once the muscle is removed the vermilion flap is moved outward into the V defect. To create an adequate V-shaped defect some skin should be removed along each side to prevent the V from being too small or thin to allow for adequate vermilion show of the mouth corner. (which naturally has the thinnest vermilion show than any other part of the lips) A two later closure is then done of the dermis/muscle and skin.
Once the muscle is removed the vermilion flap is moved outward into the V defect. To create an adequate V-shaped defect some skin should be removed along each side to prevent the V from being too small or thin to allow for adequate vermilion show of the mouth corner. (which naturally has the thinnest vermilion show than any other part of the lips) A two later closure is then done of the dermis/muscle and skin.
Aesthetic mouth widening has three potential adverse postoperative complications…scarring, relapse and an unnatural mouth corner shape. Surgical technique has an impact on all of them. Recognizing that the mouth is ringed by muscle and that for the mouth corner is to be widened then some muscle must also be removed. This gives the new mouth corner space to be repositioned with less tension which reduces the risks of all three adverse postoperative concerns.
Dr. Barry Eppley
World-Renowned Plastic Surgeon