

The lower midface consists of the central pyriform aperture or the bone around the base of the nose. Its forward development plays a major role in the projection of the nose and how the nose appears in relation to the upper lip. It is the most projecting part of the central midface where the rest of the maxillary bone is concave in shape.

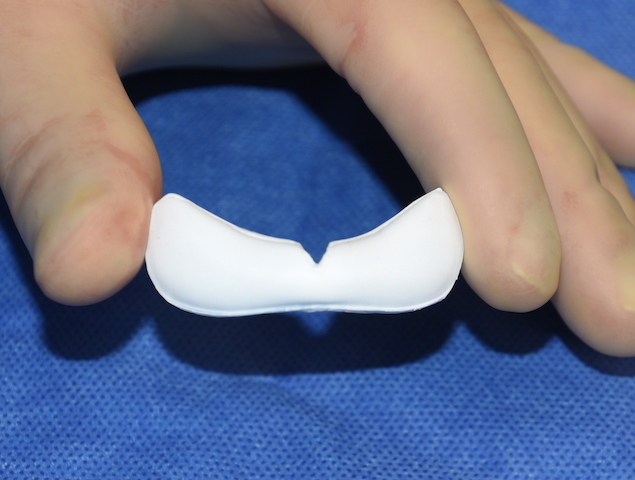
 Augmentation of the pyriform aperture region has been done by a variety of implant materials and shapes over the years but none of them have been consistently satisfactory. Getting a complete augmentation under the base of the nose that adapts well to the contours of the bone is the key. The newer ePTFE (expanded polytetrafluorethylene) midface implants is an innovation for augmentation in this facial area. It offers a good shape that is very adaptable to the bone and allows tissue ingrowth due to its microfibrillar surface structure.
Augmentation of the pyriform aperture region has been done by a variety of implant materials and shapes over the years but none of them have been consistently satisfactory. Getting a complete augmentation under the base of the nose that adapts well to the contours of the bone is the key. The newer ePTFE (expanded polytetrafluorethylene) midface implants is an innovation for augmentation in this facial area. It offers a good shape that is very adaptable to the bone and allows tissue ingrowth due to its microfibrillar surface structure.
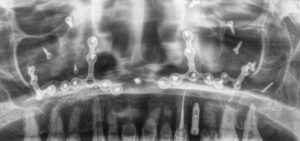 There are two ways to place the ePTFE midface implant, either through the mouth (intraoral) and through the nose. (intranasal) Each approach has its advantages and disadvantages but either one works well with good technique. The intraoral approach would be the preferred method in the patient who has had a prior LeFort I osteotomy due to the scar tissue and plate and screw hardware that would be present from the prior procedure. In addition an existing vestibular scar would already exist under the upper lip.
There are two ways to place the ePTFE midface implant, either through the mouth (intraoral) and through the nose. (intranasal) Each approach has its advantages and disadvantages but either one works well with good technique. The intraoral approach would be the preferred method in the patient who has had a prior LeFort I osteotomy due to the scar tissue and plate and screw hardware that would be present from the prior procedure. In addition an existing vestibular scar would already exist under the upper lip.
 Using the central part of the existing intraoral vestibular scarsubperiosteal undermining is done around the base of the nose. It is important to leave a good inferior cuff and muscle and mucosa on the bottom side of this incision for closure after implant placement. One can choose to remove any plates and screws that can seen with one caveat…be wary of hardware removal over the maxillary sinus as this may create a source of postoperative implant infection.
Using the central part of the existing intraoral vestibular scarsubperiosteal undermining is done around the base of the nose. It is important to leave a good inferior cuff and muscle and mucosa on the bottom side of this incision for closure after implant placement. One can choose to remove any plates and screws that can seen with one caveat…be wary of hardware removal over the maxillary sinus as this may create a source of postoperative implant infection.
 The implant comes in 5 and 6mms thicknesses which are adequate for the vast majority of patient augmentation needs. The implant is soaked in an antibiotic/betadine/phase one solution and then positioned. It has some flexibility so it can be contoured to the bone by digital manipulation. One can use a small self-tapping screw per side but most of the time this is not necessary.
The implant comes in 5 and 6mms thicknesses which are adequate for the vast majority of patient augmentation needs. The implant is soaked in an antibiotic/betadine/phase one solution and then positioned. It has some flexibility so it can be contoured to the bone by digital manipulation. One can use a small self-tapping screw per side but most of the time this is not necessary.
 Closure consists of an important two layer closure. First the muscle layer is closed ensuring that no part of the implant can be seen through it. A second outer mucosal layer is then done.
Closure consists of an important two layer closure. First the muscle layer is closed ensuring that no part of the implant can be seen through it. A second outer mucosal layer is then done.
 The effects of the nasal base augmentation are immediate. There will be some after surgery swelling but a lot of it will be gone before the first month after surgery. Patients report very little pain although most patients will experience some temporal upper lip/midfacial skin numbness but this always resolves. The one postoperative issue that takes the longest to improve is stiffness when smiling. But because the implant is below all soft tissue layers the muscles of facial expression will return to normal movement.
The effects of the nasal base augmentation are immediate. There will be some after surgery swelling but a lot of it will be gone before the first month after surgery. Patients report very little pain although most patients will experience some temporal upper lip/midfacial skin numbness but this always resolves. The one postoperative issue that takes the longest to improve is stiffness when smiling. But because the implant is below all soft tissue layers the muscles of facial expression will return to normal movement.
Of all the standard central midface implants I have ever used, this ePTFE style is the one that works the best to date n my hands. Short of a custom implant design it offer good adaptability and reshaping (trimming) if necessary.
Dr. Barry Eppley
Indianapolis, Indiana