


 The custom infraorbital-malar implant is the definitive midfacial augmentation procedure of the eyes and cheeks. By creating a horizontal line of augmentation from under the eyes and extending out onto the zygomatic arch, it establishes a distinct high cheek bone look as well as improves undereye hollows. Between the size of the implant and the relative thinness of tissues in this part of the face, this area of facial augmentation underscores the concept of a ‘little bit can go a long way.’ Custom infraorbital-malar implants are very rarely ever revised because they are too small or lack enough of an effect. Almost all revisions are done due to too profound of an effect.
The custom infraorbital-malar implant is the definitive midfacial augmentation procedure of the eyes and cheeks. By creating a horizontal line of augmentation from under the eyes and extending out onto the zygomatic arch, it establishes a distinct high cheek bone look as well as improves undereye hollows. Between the size of the implant and the relative thinness of tissues in this part of the face, this area of facial augmentation underscores the concept of a ‘little bit can go a long way.’ Custom infraorbital-malar implants are very rarely ever revised because they are too small or lack enough of an effect. Almost all revisions are done due to too profound of an effect.
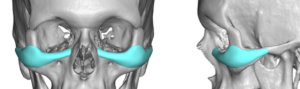
 One of the great advantages of the custom infraorbital-malar implant is its connected design across different bony areas. Just like the custom jawline implant it augments the long bony line across the flat/convex upper midface minus the central nasal area. One of its important features is that it can be designed to saddle the infraorbital rim, a key element in improving under eye hollows. It also can go way out onto the end of the zygomatic arch if desired unlike any standard cheek implant.
One of the great advantages of the custom infraorbital-malar implant is its connected design across different bony areas. Just like the custom jawline implant it augments the long bony line across the flat/convex upper midface minus the central nasal area. One of its important features is that it can be designed to saddle the infraorbital rim, a key element in improving under eye hollows. It also can go way out onto the end of the zygomatic arch if desired unlike any standard cheek implant.
The one piece infraorbital-malar implant creates a smooth linear effect unlike trying to augment these bony areas with standard infraorbital or cheek implants. But how to place such an elongated midface implant raises the debate whether it should done from an inferior intraoral approach or from a more direct lower eyelid incision. While it is certainly possible to place it from intraoral incisions there is a much higher risk of malposition, causing protracted infraorbital nerve numbness and an increased risk of infection. All of these risk factors are substantially lessened when done from the eyelid where a more horizontal line of dissection and placement can be done.
The ability to place it the one piece infraorbital-malar requires that is not completely rigid and has some bend to the material. This allows it to be placed through a partial lower eyelid incision without undue stretch and trauma to the delicate lower eyelid tissues. This elastic deformation property allows this flexion with a return to its original shape without material damage once the flexion of the implant has ceased. Only solid silicone has this property of all facial implant materials. It is often thought that a semi-rigid material is soft and won’t feel like bone….but this is not true.

 In using the lower eyelid incision for the placement of custom infraorbital-malar implant, it is important to prevent as much intraoperative bleeding and postoperative oozing as possible. Unlike other parts of the face where implants are placed, postoperative bruising with dissection around the eyes can be very significant. Such bruising can take a long time to resolve and runs the risk of refractory heme staining of the eyelid tissues. To help prevent this potential problem the lower eyelid incision is infiltrated with a 1:50,000 epinephrine solution as well as the patient is given an initial IV dose of TXA. (tranexamic acid) The eyes are protected by the placement of ophthalmic ointment with an overlying metal corneal shield. The lower eyelid incision is started with a very small lateral canthal incision of a few millimeters. It is then carried across the lower eyelid 1mm below the lash line. It usually does not need to extend much beyond the central part of the lower eyelid.
In using the lower eyelid incision for the placement of custom infraorbital-malar implant, it is important to prevent as much intraoperative bleeding and postoperative oozing as possible. Unlike other parts of the face where implants are placed, postoperative bruising with dissection around the eyes can be very significant. Such bruising can take a long time to resolve and runs the risk of refractory heme staining of the eyelid tissues. To help prevent this potential problem the lower eyelid incision is infiltrated with a 1:50,000 epinephrine solution as well as the patient is given an initial IV dose of TXA. (tranexamic acid) The eyes are protected by the placement of ophthalmic ointment with an overlying metal corneal shield. The lower eyelid incision is started with a very small lateral canthal incision of a few millimeters. It is then carried across the lower eyelid 1mm below the lash line. It usually does not need to extend much beyond the central part of the lower eyelid.
The key to working through a small eyelid incision is the use of loupe magnification, a headlight and needlepoint electrocautery. As far as can be seen the periosteum is released by the electrocautery as there are numerous perforating vessels coming from the bone which can create bothersome bleeding and contribute postoperative bruising. The only part where this can not be done is out onto the zygomatic arch which has to be done by blunt elevator dissection. But fortunately this thin bone has no perforating vessels.
 Once the pocket is made on one side, I place a TXA impregnated cottonoid sponge into it while the other side is being developed. The implants are the inserted and secured with a single screw into the cheekbone. In some cases a small screw can also be placed into the infraorbital section of the implant as well.
Once the pocket is made on one side, I place a TXA impregnated cottonoid sponge into it while the other side is being developed. The implants are the inserted and secured with a single screw into the cheekbone. In some cases a small screw can also be placed into the infraorbital section of the implant as well.
Closure of the lower eyelid incision is important as the corner of the eye is a very unforgiving area. Resuspension of the cheek tissues, a lateral canthopexy and orbicularis muscle reapposition are the key maneuvers. Unlike older blepharoplasty incisions the risk of a lower eyelid deformity is very low as it is being used for access only (no excision of tissues), support is being added, and most patients who have this surgery are young without lid laxity.
Dr. Barry Eppley
Indianapolis, Indiana