


 A custom jawline implant offers a 3D augmentation effect on the lower face. Since it is a wrap around implant, the largest aesthetic implant that can be placed on the face, its covers the entire inferolaterakl surface area of the lower jaw. In essence it is like placing a new jaw on top of the existing jaw.
A custom jawline implant offers a 3D augmentation effect on the lower face. Since it is a wrap around implant, the largest aesthetic implant that can be placed on the face, its covers the entire inferolaterakl surface area of the lower jaw. In essence it is like placing a new jaw on top of the existing jaw.
Placing such a large implant in an aesthetic manner requires adherence to two basic principles. First keep the access incisions as small as possible. Secondly avoid injuring neurovascular and muscle tissues that are along the path of dissection in making the implant pocket. Adhering to these principles requires an implant that is ‘cooperative’. A cooperative implant is one that helps in the process of ensuring these two placement principles are followed as much as possible.
 The placement of a custom jawline implant initially looks daunting when comparing the size of the incisions to that of the implant. It almost always require the use of three incisions, one anterior (chin) and posterior iintraoral incisions over the jaw angles. The chin incision can be either intraoral or through the submental skin. But it is usually far better to go submental to lower the risk of infection and to stay below the level of the bony exit of the mental nerve in the lateral chin area. There are some exceptions to the anterior submental incision. (e.g., small female jawline implants, custom jawline implants combined with sliding genioplasties) The intraoral posterior incisions can only be avoided if the jawline implant is really an extended chin implant that does not cross over into the attachments of the masseter muscle near the jaw angles.
The placement of a custom jawline implant initially looks daunting when comparing the size of the incisions to that of the implant. It almost always require the use of three incisions, one anterior (chin) and posterior iintraoral incisions over the jaw angles. The chin incision can be either intraoral or through the submental skin. But it is usually far better to go submental to lower the risk of infection and to stay below the level of the bony exit of the mental nerve in the lateral chin area. There are some exceptions to the anterior submental incision. (e.g., small female jawline implants, custom jawline implants combined with sliding genioplasties) The intraoral posterior incisions can only be avoided if the jawline implant is really an extended chin implant that does not cross over into the attachments of the masseter muscle near the jaw angles.
The reality is that these three small access incisions requires getting this large jawline implant not only through it but into the proper position (as per the design) with limited visibility of how the implant is sitting on the bone. Its success depends partially on the implant’s physical characteristics and a learned skill in doing it. Custom jawline implants can be made of various materials (silicone, Medpor, PEEk, titanium) and, while it is the patient’s choice of what they prefer, the material choices will influence how easily, successful and the scar burden needs to place it. (as well as the size of the implant design)



 The reason that solid silicone is most commonly used for custom jawline implants is both for cost (in the USA) and placement (and removal) reasons. Its elastic deformation properties allow it to change its shape to fit through the submental incision. Once all three incisions are made and general subperiosteal dissection has been completed, the jaw angle portion are passed underneath the mental nerve in a bilateral fashion. This has to be done one side at a time. This leaves the chin portion of the implant outside off the incision.
The reason that solid silicone is most commonly used for custom jawline implants is both for cost (in the USA) and placement (and removal) reasons. Its elastic deformation properties allow it to change its shape to fit through the submental incision. Once all three incisions are made and general subperiosteal dissection has been completed, the jaw angle portion are passed underneath the mental nerve in a bilateral fashion. This has to be done one side at a time. This leaves the chin portion of the implant outside off the incision.
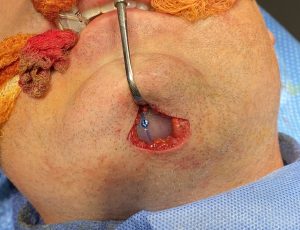 Then by pulling the posterior ends of the implant (jaw angles) back into position using the intraoral incisions the chin portion of the implant pops through the small submental incision. The chin portion is then positioned in the midline using the vertical midline marker and secured with a single midline screw.
Then by pulling the posterior ends of the implant (jaw angles) back into position using the intraoral incisions the chin portion of the implant pops through the small submental incision. The chin portion is then positioned in the midline using the vertical midline marker and secured with a single midline screw.
Once the anterior position of the jawline implant is established this allows the posterior jaw angle portions of the implant to be stretched out to length and positioned. (a little bit like laying carpet) In other words establishing the central position of the implant allows the two sides to the properly stretched out. In the deep intraoral region of the jaw angles not getting the implant to length is the most common cause of implant malposition.
Dr. Barry Eppley
World-Renowned Plastic Surgeon