


Jaw angle implants have been around for over twenty-five years but were very infrequently used. They have had a more recent resurgence of aesthetic relevance due to the contemporary emphasis for a more visible and defined jawline, improved jaw angle implant styles and the widespread use of injectable augmentation strategies. (synthetic fillers and fat)
Jaw angle implants have traditionally been associated with men and the desire for a strong jawline. While this still remains true an improved jawline can be an equal female desire as well. No longer is a good jawline an exclusive male aesthetic desire..

 While females undergo today an increasing number of jaw angle augmentations, it is important to recognize their aesthetic differences from that of men. While men frequently need a jaw angle widening effect, this is rarely the case in women. Women seek jaw angle augmentation most of the time because they have a high and indistinct jaw angle shape with a steeper mandibular plane angle. Most women with well defined jaw angles have less wide jawlines with a more vertical component. Thus most of the time the vertical lengthening style of jaw angle implant is needed for women.
While females undergo today an increasing number of jaw angle augmentations, it is important to recognize their aesthetic differences from that of men. While men frequently need a jaw angle widening effect, this is rarely the case in women. Women seek jaw angle augmentation most of the time because they have a high and indistinct jaw angle shape with a steeper mandibular plane angle. Most women with well defined jaw angles have less wide jawlines with a more vertical component. Thus most of the time the vertical lengthening style of jaw angle implant is needed for women.
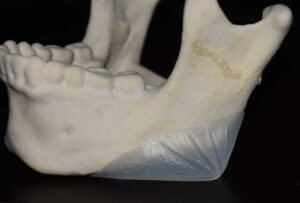
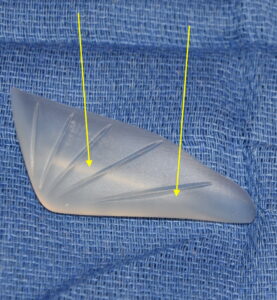 Think of the vertical lengthening jaw angle implant as adding a ‘cap’ to the jaw angle which lacks definition. It drops it down and in so doing creates a visible jaw angle shape. This is apparent on the internal side of the implant which has a ledge onto which the inferior border of the existing jaw angle bone is to sit.
Think of the vertical lengthening jaw angle implant as adding a ‘cap’ to the jaw angle which lacks definition. It drops it down and in so doing creates a visible jaw angle shape. This is apparent on the internal side of the implant which has a ledge onto which the inferior border of the existing jaw angle bone is to sit.
Surgical Technique
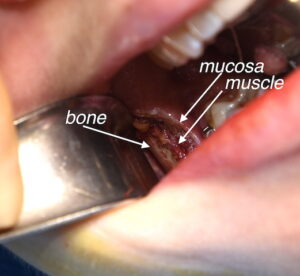 The intraoral approach uses a posterior vestibular incision. The key to this incision is placement. It follows the underlying external oblique line opposite the molar teeth. By so doing this leaves a healthy cuff of tissue on the inner side which is critical for a competent two layer closure after the implant is placed.
The intraoral approach uses a posterior vestibular incision. The key to this incision is placement. It follows the underlying external oblique line opposite the molar teeth. By so doing this leaves a healthy cuff of tissue on the inner side which is critical for a competent two layer closure after the implant is placed.
 A subperiosteal pocket is created back to the posterior border and down to the inferior border of the jaw angle bone. At this point one may think that the pocket dissection is done….but this is the easy part. What one has to do next is the critical part, the gentle subperiosteal dissection at and under the inferior border back around the bony jaw angle up along the inferior border. This requires the release of the osteocutaneous ligaments of the jaw angle which is some patients are very tenous while in others they are less adherent. Almost all women had less adherent ligamentous attachments than men. These ligaments must be carefully elevated off the bone to keep the masseteric sling intact along the inferior border up to the midbody of the mandible. Without this part of the dissection the jaw angle implant is never going to fit properly as the lower part of the implant must wrap around the inferior border to create a new jaw angle.
A subperiosteal pocket is created back to the posterior border and down to the inferior border of the jaw angle bone. At this point one may think that the pocket dissection is done….but this is the easy part. What one has to do next is the critical part, the gentle subperiosteal dissection at and under the inferior border back around the bony jaw angle up along the inferior border. This requires the release of the osteocutaneous ligaments of the jaw angle which is some patients are very tenous while in others they are less adherent. Almost all women had less adherent ligamentous attachments than men. These ligaments must be carefully elevated off the bone to keep the masseteric sling intact along the inferior border up to the midbody of the mandible. Without this part of the dissection the jaw angle implant is never going to fit properly as the lower part of the implant must wrap around the inferior border to create a new jaw angle.
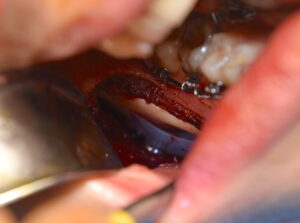 When placing the implant it must look parallel to the bone when viewed through the incision. This means the inferior portion of the implant, which has a ledge on its inner surface, is down properly and in good position. Sometimes this almost ‘snaps’ into place but more commonly you have to see that the upper part of the implant goes completely down vertically. When in good position a visible jaw angle will be seen on the outside and by feel a new jaw angle will be felt. The old jaw angle should no longer be palpable as it is covered by the implant.
When placing the implant it must look parallel to the bone when viewed through the incision. This means the inferior portion of the implant, which has a ledge on its inner surface, is down properly and in good position. Sometimes this almost ‘snaps’ into place but more commonly you have to see that the upper part of the implant goes completely down vertically. When in good position a visible jaw angle will be seen on the outside and by feel a new jaw angle will be felt. The old jaw angle should no longer be palpable as it is covered by the implant.


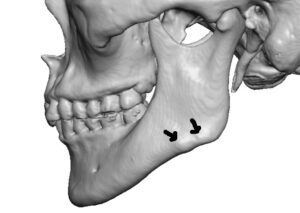
 Once the implant is in position screw fixation is essential. If not the implant will displace upward and the jaw angle effect will be lost. (and worse…an asymmetric widening effect will occur) The two key components of jaw angle screw fixation are: 1) a percutaneous technique is needed (don’t even try going through the mouth as it is completely the wrong angle for such a low positioned implant), 2) 2.0mm self-tapping screws are used (4 to 5mms in length) one or two per side.These are loaded onto the screw driver inside the mouth after having passed perpendicular to the jaw through the masseter muscle with a 2mm external skin nick. This is the fastest and more secure method of jaw angle implant screw fixation.
Once the implant is in position screw fixation is essential. If not the implant will displace upward and the jaw angle effect will be lost. (and worse…an asymmetric widening effect will occur) The two key components of jaw angle screw fixation are: 1) a percutaneous technique is needed (don’t even try going through the mouth as it is completely the wrong angle for such a low positioned implant), 2) 2.0mm self-tapping screws are used (4 to 5mms in length) one or two per side.These are loaded onto the screw driver inside the mouth after having passed perpendicular to the jaw through the masseter muscle with a 2mm external skin nick. This is the fastest and more secure method of jaw angle implant screw fixation.
After antibiotic irrigation a two layer closure is done of both muscle and mucosa with 3-0 chromic running suture. A competent two layer closure is important for a watertight seal of thick tissue over the implant.
Jaw angle implants of any shape or size are the most challenging of all standard facial implants for placement due to the more remote posterior intraoral approach, lack of visibility of the working end of the implant and the need for screw fixation. This is very different from the anterior chin implant which poses none of these surgical challenges. However it is a jaw implant procedure that can be successfully performed by following these learned techniques.
Dr. Barry Eppley
Indianapolis, Indiana