

Shoulder width reduction by reducing the length of the clavicle is a very effective upper body reshaping procedure. In a near 1:1 relationship with the amount of clavicle removed, the bideltoid width of the shoulders is reduced. The result is immediate and is unaffected by any swelling that occurs at the actual site of the bone removal. (which is at the opposite end of the clavicle)
 Integral to any type of elective clavicle surgery (reduction or lengthening) is plate and screw fixation. Without stable fixation the clavicle osteotomy site will be unstable, become misaligned and will likely end up as a non-union. The techniques for plate and screw fixation of the clavicle comes from fracture repair. The clavicle is a commonly fractured bone and many different methods have been used to realign and stabilize it. Four types of 2.7mm or 3.5mm fixation plates have been used in clavicle fracture repair including reconstruction, locking reconstruction, dynamic compression and locking compression plates. Based on comminuted mid shaft fracture repairs reconstruction plates have higher failure rates than non-reconstruction plates.
Integral to any type of elective clavicle surgery (reduction or lengthening) is plate and screw fixation. Without stable fixation the clavicle osteotomy site will be unstable, become misaligned and will likely end up as a non-union. The techniques for plate and screw fixation of the clavicle comes from fracture repair. The clavicle is a commonly fractured bone and many different methods have been used to realign and stabilize it. Four types of 2.7mm or 3.5mm fixation plates have been used in clavicle fracture repair including reconstruction, locking reconstruction, dynamic compression and locking compression plates. Based on comminuted mid shaft fracture repairs reconstruction plates have higher failure rates than non-reconstruction plates.

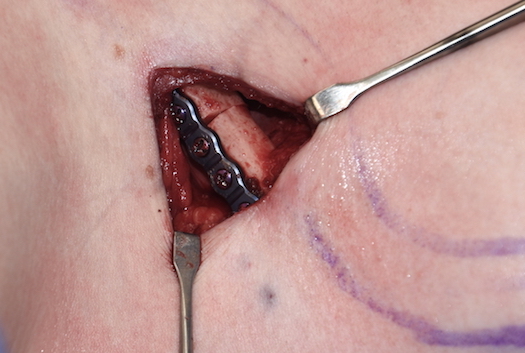
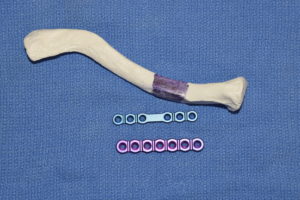
 But comminuted fractures at the middle part of the clavicle is different than a clean transverse osteotomy at the thicker medial third of the bone which is done in shoulder width reduction surgery. The end to end apposition is more structurally stable and any plate application, regardless of the plate type, is more solid. Reconstruction plates have a lower profile with notched edges that better fit the surface of the bone. So even though they have less plate stiffness than non-reconstruction plates they appear to be adequate in my experience to date. In addition the use of a six-hole plate with three bicortical screws per side also seems to be sufficient.
But comminuted fractures at the middle part of the clavicle is different than a clean transverse osteotomy at the thicker medial third of the bone which is done in shoulder width reduction surgery. The end to end apposition is more structurally stable and any plate application, regardless of the plate type, is more solid. Reconstruction plates have a lower profile with notched edges that better fit the surface of the bone. So even though they have less plate stiffness than non-reconstruction plates they appear to be adequate in my experience to date. In addition the use of a six-hole plate with three bicortical screws per side also seems to be sufficient.
 The application of the plate on the superior surface of the bone has been shown in fracture repair to provide the best resistance to deforming forces. That is also the approach I take in reduction osteotomies as that concept is supported by numerous biomechanical studies. When in doubt application of an additional plate on the anterior surface can also be done for maximal resistance to rotational forces.
The application of the plate on the superior surface of the bone has been shown in fracture repair to provide the best resistance to deforming forces. That is also the approach I take in reduction osteotomies as that concept is supported by numerous biomechanical studies. When in doubt application of an additional plate on the anterior surface can also be done for maximal resistance to rotational forces.
Given that in shoulder width reduction both clavicles undergo the same procedure, it may be that a lesser amount of plate fixation is needed due to limited movement of both arms. (which is not what exists in clavicle fractures) But until further biomechanical studies are done, or different plates are designed, the single row six-hole plate will continue to be used.
Dr. Barry Eppley
Indianapolis, Indiana