


The lateral canthoplasty is a well known procedure that has value in both reconstructive (e.g., ectropion) and aesthetic eyelid surgery. (e.g., cat eye surgery) While once originally described as reattaching the lateral canthal tendon to the periosteum inside the lateral orbital rim, it has evolved today to use a direct attachment to the bone using sutures passed through drill holes. This more effectively raises the corner of the eye and provides better long term retention of its position.
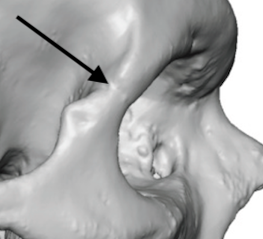
One of the interesting questions about lateral canthoplasy is where should the drill holes be placed and what is the best way to get there. A good reference is the frontozygomatic suture which is the anatomic demarcation between the brow bone and the lateral orbital rim. The normal position of the lateral canthal tendon attachment to the bone is below this suture line, sometimes well below it based on the natural position of the lateral eye corner.
 As a general rule, the position of the drill holes should be at or above the frontozygomatic suture. The greater the degree of corner elevation desired the higher the drill holes should be placed. Double drill holes should always be used which allows the suture to pull the tendon reattachment inside the orbital rim. This keeps the lower eyelid up against the eyeball to prevent postoperative eye irritation/dryness. A single drill hole suture would allow the important intimate relationship between the lid and globe to be disrupted.
As a general rule, the position of the drill holes should be at or above the frontozygomatic suture. The greater the degree of corner elevation desired the higher the drill holes should be placed. Double drill holes should always be used which allows the suture to pull the tendon reattachment inside the orbital rim. This keeps the lower eyelid up against the eyeball to prevent postoperative eye irritation/dryness. A single drill hole suture would allow the important intimate relationship between the lid and globe to be disrupted.

 Once the suture is tightened the outer eye corner raises considerably. In so doing this will cause two expected soft tissue effects. First the lifted outer eye corner will tuck in under the upper lash line a bit. Unless one is doing a concurrent temporal lift in a female this effect will persist in the early postoperative period but it is not usually a permanent one. Secondly, below the raised eye corner a triangular soft tissue defect will appear. This will need to be filled in during closure by soft tissue advancement from the upper cheek into it during closure.
Once the suture is tightened the outer eye corner raises considerably. In so doing this will cause two expected soft tissue effects. First the lifted outer eye corner will tuck in under the upper lash line a bit. Unless one is doing a concurrent temporal lift in a female this effect will persist in the early postoperative period but it is not usually a permanent one. Secondly, below the raised eye corner a triangular soft tissue defect will appear. This will need to be filled in during closure by soft tissue advancement from the upper cheek into it during closure.
With placing the drill holes at or above the frontozygomatic suture line the best access is from a small upper eyelid incision in the skin crease. Trying to reach there from a lower eyelid/lateral canthal incision runs the risk of placing the drill holes too low and decreasing the effectiveness of the procedure.
Dr. Barry Eppley
Indianapolis, Indiana